<body><script type="text/javascript">
function setAttributeOnload(object, attribute, val) {
if(window.addEventListener) {
window.addEventListener('load',
function(){ object[attribute] = val; }, false);
} else {
window.attachEvent('onload', function(){ object[attribute] = val; });
}
}
</script>
<div id="navbar-iframe-container"></div>
<script type="text/javascript" src="https://apis.google.com/js/platform.js"></script>
<script type="text/javascript">
gapi.load("gapi.iframes:gapi.iframes.style.bubble", function() {
if (gapi.iframes && gapi.iframes.getContext) {
gapi.iframes.getContext().openChild({
url: 'https://www.blogger.com/navbar.g?targetBlogID\x3d4281345071830776296\x26blogName\x3dNurse\x27+Station\x26publishMode\x3dPUBLISH_MODE_BLOGSPOT\x26navbarType\x3dBLUE\x26layoutType\x3dCLASSIC\x26searchRoot\x3dhttps://nursephil.blogspot.com/search\x26blogLocale\x3den_US\x26v\x3d2\x26homepageUrl\x3dhttp://nursephil.blogspot.com/\x26vt\x3d-6681382105036761632',
where: document.getElementById("navbar-iframe-container"),
id: "navbar-iframe"
});
}
});
</script><iframe src="http://www.blogger.com/navbar.g?targetBlogID=17123322&amp;blogName=Nurse's Station&amp;publishMode=PUBLISH_MODE_BLOGSPOT&amp;navbarType=SILVER&amp;layoutType=CLASSIC&amp;homepageUrl=http%3A%2F%2Fcomperkrn.blogspot.com%2F&amp;searchRoot=http%3A%2F%2Fcomperkrn.blogspot.com%2Fsearch" marginwidth="0" marginheight="0" scrolling="no" frameborder="0" height="30px" width="100%" id="navbar-iframe"></iframe>
<div id="space-for-ie"></div>

"You are writing for your own people,
who in their silence, perhaps poverty
cannot express their aspirations and
anguish. You are their only voice
but only if you have not deserted
nor betrayed them."
--f sionil jose

www.nursephil.blogspot.com
CONCEPTS
.Psyche Nursing.
.IMCI-Lec.
.Nsg Concepts.
.Medical-Surgical.
.Fundamentals.
.Community.
.Pedia.
.Prof Adjustment/Research/Mgt.

PRATICE EXAM
.Test Taking Tips
.Psyche Exam
.Pedia Exam
.Prof Ad Exam
.Medical-Surgical Exam
.Fundamentals Exam
.OB Exam
.Pharma Exam
Contact Us
comperk_rn@yahoo.com
aln_rn@yahoo.com
this blog is kinda new
so please bear with us
email us with your
comments
suggestions
and informations
we'll be glad to
post it for you
Nursing Exam Secrets
The 5 Secret Keys to Nursing Exam Success:
• Time is Your Greatest Enemy
• Guessing is Not Guesswork
• Practice Smarter, Not Harder
• Prepare, Don't Procrastinate
• Test Yourself
A comprehensive Word Knowledge Review covering:
• Nearly and Perfect Synonyms
• Prefixes
• Positive vs. Negative
• Word Strength
• Type and Topic
• Form a Sentence
• Use Replacements
• Eliminate Similar Choices
• Adjectives Give it Away
• Use Logic
• The Trap of Familiarity
A comprehensive General Strategy review with:
• Make Predictions
• Answer the Question
• Benchmark
• Valid Information
• Avoid "Fact Traps"
• Milk the Question
• The Trap of Familiarity
• Eliminate Answers
• Tough Questions
• Brainstorm
• Read Carefully
• Face Value
• Prefixes
• Hedge Phrases
• Switchback Words
• New Information
• Time Management
• Contextual Clues
• Don't Panic
• Pace Yourself
• Answer Selection
• Check Your Work
• Beware of Directly Quoted Answers
• Slang
• Extreme Statements
• Answer Choice Families
A comprehensive Medical Review covering:
• Nervous System
• Signs and Symptoms
• Major Hormones
• Respiratory System
• Cardiac Review
• Breathing Sounds
• Proper Medication
• Maternal Responses
• Psychological Processes
• Blood and Urine Values
• Developmental Milestones
• Organ Functions
• Burn and Wound Care
A comprehensive Pharmacology Review covering:
• Cholinomimetrics
• Anticholinergics
• Adrenegic Agonists
• Adrenergic Antagonists
• Centrally Acting Agents
• Direct Acting Relaxants
• Neuromuscular Junction Blockers
• Other Muscle Relaxants
• Local Anesthetics
• General Anesthetics
• Sedative Hypnotics
• Antianxiety Agents
• Affective Disorders
• Antipsychotics
• Seizures
• Opioids
• Non-opioid Analgesics
• Anti-inflammatory Drugs
• Respiratory Pharmacology
• GI Pharmacology
• Cardiovascular Pharmacology
• Coagulation Disorders
• Hyperlipidemia
• Diabetes Mellitus
Pediatric Nursing Exam
Situation 1: Raphael, a 6 year’s old prep pupil is seen at the school clinic for growth and development monitoring (Questions 1-5)
1. Which of the following is characterized the rate of growth during this period?
a. most rapid period of growth
b. a decline in growth rate
c. growth spurt
d. slow uniform growth rate
2. In assessing Raphael’s growth and development, the nurse is guided by principles of growth and development. Which is not included?
a. All individuals follow cephalo-caudal and proximo-distal
b. Different parts of the body grows at different rate
c. All individual follow standard growth rate
d. Rate and pattern of growth can be modified
3. What type of play will be ideal for Raphael at this period?
a. Make believe
b. Hide and seek
c. Peek-a-boo
d. Building blocks
4. Which of the following information indicate that Raphael is normal for his age?
a. Determine own sense self
b. Develop sense of whether he can trust the world
c. Has the ability to try new things
d. Learn basic skills within his culture
5. Based on Kohlberg’s theory, what is the stage of moral development of Raphael?
a. Punishment-obedience
b. “good boy-Nice girl”
c. naïve instrumental orientation
d. social contact
Situation 2 Baby boy Lacson delivered at 36 weeks gestation weighs 3,400 gm and height of 59 cm (6-10)
6. Baby boy Lacson’s height is
a. Long
b. Short
c. Average
d. Too short
7. Growth and development in a child progresses in the following ways EXCEPT
a. From cognitive to psychosexual
b. From trunk to the tip of the extremities
c. From head to toe
d. From general to specific
8. As described by Erikson, the major psychosexual conflict of the above situation is
a. Autonomy vs. Shame and doubt
b. Industry vs. Inferiority
c. Trust vs. mistrust
d. Initiation vs. guilt
9. Which of the following is true about Mongolian Spots?
a. Disappears in about a year
b. Are linked to pathologic conditions
c. Are managed by tropical steroids
d. Are indicative of parental abuse
10. Signs of cold stress that the nurse must be alert when caring for a Newborn is:
a. Hypothermia
b. Decreased activity level
c. Shaking
d. Increased RR
Situation 3 Nursing care after delivery has an important aspect in every stages of delivery
11. After the baby is delivered, the cord was cut between two clamps using a sterile scissors and blade, then the baby is placed at the:
a. Mother’s breast
b. Mother’s side
c. Give it to the grandmother
d. Baby’s own mat or bed
12. The baby’s mother is RH(-). Which of the following laboratory tests will probably be ordered for the newborn?
a. Direct Coomb’s
b. Indirect Coomb’s
c. Blood culture
d. Platelet count
13. Hypothermia is common in newborn because of their inability to control heat. The following would be an appropriate nursing intervention to prevent heat loss except
a. Place the crib beside the wall
b. Doing Kangaroo care
c. By using mechanical pressure
d. Drying and wrapping the baby
14. The following conditions are caused by cold stress except
a. Hypoglycemia
b. Increase ICP
c. Metabolic acidosis
d. Cerebral palsy
15. During the feto-placental circulation, the shunt between two atria is called
a. Ductus venosous
b. Foramen Magnum
c. Ductus arteriosus
d. Foramen Ovale
16. What would cause the closure of the Foramen ovale after the baby had been delivered?
a. Decreased blood flow
b. Shifting of pressures from right side to the left side of the heart
c. Increased PO2
d. Increased in oxygen saturation
17. Failure of the Foramen Ovale to close will cause what Congenital Heart Disease?
a. Total anomalous Pulmunary Artery
b. Atrial Septal defect
c. Transposition of great arteries
d. Pulmunary Stenosis
Situation 4 Children are vulnerable to some minor health problems or injuries hence the nurse should be able to teach mothers to give appropriate home care.
18. A mother brought her child to the clinic with nose bleeding. The nurse showed the mother the most appropriate position for the child which is:
a. Sitting up
b. With low back rest
c. With moderate back rest
d. Lying semi flat
19. A common problem in children is the inflammation of the middle ear. This is related to the malfunctioning of the:
a. Tympanic membrane
b. Eustachian tube
c. Adenoid
d. Nasopharynx
20. For acute otitis media, the treatment is prompt antibiotic therapy. Delayed treatment may result in complications of:
a. Tonsillitis
b. Eardrum Problems
c. Brain damage
d. Diabetes mellitus
21. When assessing gross motor development in a 3 year old, which of the following activities would the nurse expect to finds?
a. Riding a tricycle
b. Hopping on one foot
c. Catching a ball
d. Skipping on alternate foot.
22. When assessing the weight of a 5-month old, which of the following indicates healthy growth?
a. Doubling of birth weight
b. Tripling of birth weight
c. Quadrupling of birth weight
d. Stabilizing of birth weight
23. An appropriate toy for a 4 year old child is:
a. Push-pull toys
b. Card games
c. Doctor and nurse kits
d. Books and Crafts
24. Which of the following statements would the nurse expects a 5-year old boy to say whose pet gerbil just died
a. “The boogieman (kamatayan- the man with the scythe) got him”
b. “He’s just a bit dead”
c. “Ill be good from now own so I wont die like my gerbil”
d. “Did you hear the joke about…”
25. When assessing the fluid and electrolyte balance in an infant, which of the following would be important to remember?
a. Infant can concentrate urine at an adult level
b. The metabolic rate of an infant is slower than in adults
c. Infants have more intracellular water that adult do
d. Infant have greater body surface area than adults
26. When assessing a child with aspirin overdose, which of the following will be expected?
a. Metabolic alkalosis
b. Respiratory alkalosis
c. Metabolic acidosis
d. Respiratory acidosis
27. Which of the following is not a possible systemic clinical manifestation of severe burns?
a. Growth retardation
b. Hypermetabolism
c. Sepsis
d. Blisters and edema
28. When assessing a family for potential child abuse risks, the nurse would observe for which of the following?
a. Periodic exposure to stress
b. Low socio-economic status
c. High level of self esteem
d. Problematic pregnancies
29. Which of the following is a possible indicator of Munchausen syndrome by proxy type of child abuse?
a. Bruises found at odd locations, with different stages of healing
b. STD’s and genital discharges
c. Unexplained symptoms of diarrhea, vomiting and apnea with no organic basis
d. Constant hunger and poor hygiene
30. Which of the following is an inappropriate interventions when caring for a child with HIV?
a. Teaching family about disease transmission
b. Offering large amount of fresh fruits and vegetables
c. Encouraging child to perform at optimal level
d. Teach proper hand washing technique
Situation 5 Agata, 2 years old is rushed to the ER due to cyanosis precipitated by crying. Her mother observed that after playing she gets tired. She was diagnosed with Tetralogy of Fallot.
31. The goal of nursing care fro Agata is to:
a. Prevent infection
b. Promote normal growth and development
c. Decrease hypoxic spells
d. Hydrate adequately
32. The immediate nursing intervention for cyanosis of Agata is:
a. Call up the pediatrician
b. Place her in knee chest position
c. Administer oxygen inhalation
d. Transfer her to the PICU
33. Agata was scheduled for a palliative surgery, which creates anastomosis of the subclavian artery to the pulmonary artery. This procedure is:
a. Waterston-Cooley
b. Raskkind Procedure
c. Coronary artery bypass
d. Blalock-Taussig
34. Which of the following is not an indicator that Agata experiences separation anxiety brought about her hospitalization?
a. Friendly with the nurse
b. Prolonged loud crying, consoled only by mother
c. Occasional temper tantrums and always says NO
d. Repeatedly verbalizes desire to go home
35. When Agata was brought to the OR, her parents where crying. What would be the most appropriate nursing diagnosis?
a. Infective family coping r/t situational crisis
b. Anxiety r/t powerlessness
c. Fear r/t uncertain prognosis
d. Anticipatory grieving r/t gravity of child’s physical status
36. Which of the following respiratory condition is always considered a medical emergency?
a. Laryngeotracheobronchitis (LTB)
b. Epiglottitis
c. Asthma
d. Cystic Fibrosis
37. Which of the following statements by the family of a child with asthma indicates a need for additional teaching?
a. “We need to identify what things triggers his attacks”
b. “He is to use bronchodilator inhaler before steroid inhaler”
c. “We’ll make sure he avoids exercise to prevent asthma attacks”
d. “he should increase his fluid intake regularly to thin secretions”
38. Which of the following would require careful monitoring in the child with ADHD who is receiving Methylphenidate (Ritalin)?
a. Dental health
b. Mouth dryness
c. Height and weight
d. Excessive appetite
Situation 6 Laura is assigned as the Team Leader during the immunization day at the RHU
39. What program for the DOH is launched at 1976 in cooperation with WHO and UNICEF to reduce morbidity and mortality among infants caused by immunizable disease?
a. Patak day
b. Immunization day on Wednesday
c. Expanded program on immunization
d. Bakuna ng kabtaan
40. One important principle of the immunization program is based on?
a. Statistical occurrence
b. Epidemiologic situation
c. Cold chain management
d. Surveillance study
41. The main element of immunization program is one of the following?
a. Information, education and communication
b. Assessment and evaluation of the program
c. Research studies
d. Target setting
42. What does herd immunity means?
a. Interruption of transmission
b. All to be vaccinated
c. Selected group for vaccination
d. Shorter incubation
43. Measles vaccine can be given simultaneously. What is the combined vaccine to be given to children starting at 15 months?
a. MCG
b. MMR
c. BCG
d. BBR
Situation 7: Braguda brought her 5-month old daughter in the nearest RHU because her baby sleeps most of the time, with decreased appetite, has colds and fever for more than a week. The physician diagnosed pneumonia.
44. Based on this data given by Braguda, you can classify Braguda’s daughter to have:
a. Pneumonia: cough and colds
b. Severe pneumonia
c. Very severe pneumonia
d. Pneumonia moderate
45. For a 3-month old child to be classified to have Pneumonia (not severe), you would expect to find RR of:
a. 60 bpm
b. 40 bpm
c. 70 bpm
d. 50 pbm
46. You asked Braguda if her baby received all vaccines under EPI. What legal basis is used in implementing the UN’s goal on Universal Child Immunization?
a. PD no. 996
b. PD no. 6
c. PD no. 46
d. RA 9173
47. Braguda asks you about Vitamin A supplementation. You responded that giving Vitamin A starts when the infant reaches 6 months and the first dose is”
a. 200,000 “IU”
b. 100,000 “IU”
c. 500,000 “IU”
d. 10,000 “IU”
48. As part of CARI program, assessment of the child is your main responsibility. You could ask the following question to the mother except:
a. “How old is the child?”
b. “IS the child coughing? For how long?”
c. “Did the child have chest indrawing?”
d. “Did the child have fever? For how long?”
49. A newborn’s failure to pass meconium within 24 hours after birth may indicate which of the following?
a. Aganglionic Mega colon
b. Celiac disease
c. Intussusception
d. Abdominal wall defect
50. The nurse understands that a good snack for a 2 year old with a diagnosis of acute asthma would be:
a. Grapes
b. Apple slices
c. A glass of milk
d. A glass of cola
51. Which of the following immunizations would the nurse expect to administer to a child who is HIV (+) and severely immunocomromised?
a. Varicella
b. Rotavirus
c. MMR
d. IPV
52. When assessing a newborn for developmental dysplasia of the hip, the nurse would expect to assess which of the following?
a. Symmetrical gluteal folds
b. Trendelemburg sign
c. Ortolani’s sign
d. Characteristic limp
53. While assessing a male neonate whose mother desires him to be circumcised, the nurse observes that the neonate’s urinary meatus appears to be located on the ventral surface of the penis. The physician is notified because the nurse would suspect which of the following?
a. Phimosis
b. Hydrocele
c. Epispadias
d. Hypospadias
54. When teaching a group of parents about seat belt use, when would the nurse state that the child be safely restrained in a regular automobile seatbelt?
a. 30 lb and 30 in
b. 35 lb and 3 y/o
c. 40 lb and 40 in
d. 60 lb and 6 y/o
55. When assessing a newborn with cleft lip, the nurse would be alert which of the following will most likely be compromised?
a. Sucking ability
b. Respiratory status
c. Locomotion
d. GI function
56. For a child with recurring nephritic syndrome, which of the following areas of potential disturbances should be a prime consideration when planning ongoing nursing care?
a. Muscle coordination
b. Sexual maturation
c. Intellectual development
d. Body image
57. An inborn error of metabolism that causes premature destruction of RBC?
a. G6PD
b. Hemocystinuria
c. Phenylketonuria
d. Celiac Disease
58. Which of the following would be a diagnostic test for Phenylketonuria which uses fresh urine mixed with ferric chloride?
a. Guthrie Test
b. Phenestix test
c. Beutler’s test
d. Coomb’s test
59. Dietary restriction in a child who has Hemocystenuria will include which of the following amino acid?
a. Lysine
b. Methionine
c. Isolensine tryptophase
d. Valine
60. A milk formula that you can suggest for a child with Galactosemia:
a. Lofenalac
b. Lactum
c. Neutramigen
d. Sustagen
CLICK HERE FOR ANSWERS AND RATIONALE
PHARMACOLOGY
TEST 1
1. Which of the following is not a side effect of the cholinoreceptor blocker (Atropine)?
a. Increased pulse
b. Urinary retention
c. Constipation
d. Mydriasis
2. Which of the following is not a side effect of the Ace Inhibitor (Captopril)?
a. Rash
b. Angioedema
c. Cough
d. Congestion
3. Which of the following is not a side effect of the Vasodilator (Nifedipine)?
a. Nausea
b. Flush appearance
c. Vertigo
d. Sexual dysfunction
4. Which of the following is not a side effect of the Sympathoplegics (Clonidine)?
a. Hypertension
b. Asthma
c. Dry oral cavity
d. Lethargic behavior
5. Which of the following is not a side effect of the Dieuretics (Loop dieuretics)?
a. Alkalosis
b. Nausea
c. Hypotension
d. Potassium deficits
6. Which of the following is not an effect of the drug (Isoflurane)?
a. Elevated lipid levels
b. Nausea
c. Increased blood flow to the brain.
d. Decreased respiratory function
7. Which of the following is not an effect of the drug (Midazolam)?
a. Amnesia
b. Decreased respiratory function
c. Anesthetic
d. Dizziness
8. Which of the following is not an effect of the drug (Clozapine)?
a. Agranulocytosis
b. Antipsychotic
c. Used for Schizophrenia
d. Increased appetite
9. Which of the following is not treated with (Epinephrine)?
e. Renal disease
a. Asthma
b. Hypotension
c. Glaucoma
10. Which of the following is not treated with (Ephedrine)?
a. COPD
b. Hypotension
c. Congestion
d. Incontinence
11. Which of the following are not treated with Barbiturates?
a. Seizures
b. Hypotension
c. Insomnia
*d. Anxiety
12. Which of the following are not treated with opoid analgesics like (dextromethorphan and methadone)?
a. Pulmonary Edema
b. Cough suppression
c. Sedation
d. Pain
13. Which of the following are not treated with Hydrochlorothiazide?
a. CHF
b. HTN
c. Nephritis
d. Hypercalciuria
14. Which of the following are not treated with Nifedipine?
a. Angina
b. Arrhythmias
c. Hypertension
d. Fluid retention
16. Which of the following are not treated with Methotrexate?
a. Sarcomas
b. Leukemias
c. Ectopic pregnancy
d. Rheumatic fever
17. Which of the following are not treated with Prednisone?
a. Cushing’s disease
b. Testicular cancer
c. Lympthomas
d. Chronic leukemias
18. Which of the following are not treated with Dexamethasone?
a. Inflammation
b. Asthma
c. Addison’s disease
d. Wilson’s disease
19. Which of the following are not treated with Lansoprazole?
a. Zollinger-Ellison syndrome
b. Gastritis
c. Hypertension
d. Reflux
20. Which of the following is the antidote for the toxin Heparin?
a. Protamine
b. Methylene blue
c. N-acetylcysteine
d. Glucagon
21. Which of the following is the antidote for the toxin Copper?
a. Glucagon
b. Aminocaproic acid
c. Atropine
d. Penicillamine
PEDIATRIC NURSING Answers and Rationale
Situation 1: Raphael, a 6 year’s old prep pupil is seen at the school clinic for growth and development monitoring (Questions 1-5)
1. Which of the following is characterized the rate of growth during this period?
a. most rapid period of growth
b. a decline in growth rate
c. growth spurt
d. slow uniform growth rate
Correct answer is letter B. During the Preschooler stage growth is very minimal. Weight gain is only 4.5lbs (2kgs) per year and Height is 3.5in (6-8cm) per year.
Review:
Most rapid growth and development- Infancy
Slow growth- Toddler hood and Preschooler
Slower growth- School age
Rapid growth- Adolescence
2. In assessing Raphael’s growth and development, the nurse is guided by principles of growth and development. Which is not included?
a. All individuals follow cephalo-caudal and proximo-distal
b. Different parts of the body grows at different rate
c. All individual follow standard growth rate
d. Rate and pattern of growth can be modified
Growth and development occurs in cephalo-caudal meaning development occurs through out the body’s axis. Example: the child must be able to lift the head before he is able to lift his chest. Proximo-distal is development that progresses from center of the body to the extremities. Example: a child first develops arm movement before fine-finger movement. Different parts of the body grows at different range because some body tissue mature faster than the other such as the neurologic tissues peaks its growth during the first years of life while the genital tissue doesn’t till puberty. Also G&D is predictable in the sequence which a child normally precedes such as motor skills and behavior. Lastly G&D can never be modified
3. What type of play will be ideal for Raphael at this period?
a. Make believe
b. Hide and seek
c. Peek-a-boo
d. Building blocks
Correct answer is Letter A, make believe is most appropriate because it enhances the imitative play and imagination of the preschooler. C and D are for infants while letter A is B is recommended for schoolers because it enhances competitive play.
4. Which of the following information indicate that Raphael is normal for his age?
a. Determine own sense self
b. Develop sense of whether he can trust the world
c. Has the ability to try new things
d. Learn basic skills within his culture
The correct answer is letter C; because Erickson defines the developmental task of a preschool period is learning Initiative vs. Guilt. Children can initiate motor activities of various sorts on their own and no longer responds to or imitate the actions of other children or of their parents. Letter A and B is.. for you!!
5. Based on Kohlberg’s theory, what is the stage of moral development of Raphael?
a. Punishment-obedience
b. “good boy-Nice girl”
c. naïve instrumental orientation
d. social contact
Correct answer is letter C: According to Kohlber, a preschooler is under Pre-conventional where a child learns about instrumental purpose and exchange, that is they will something do for another if that that person does something with the child in return. Letter A is applicable for Toddlers and letter B is for a School age child.
Situation 2 Baby boy Lacson delivered at 36 weeks gestation weighs 3,400 gm and height of 59 cm (6-10)
6. Baby boy Lacson’s height is
a. Long
b. Short
c. Average
d. Too short
Correct answer is Letter A because the normal length of a newborn is 47.5-53.75 cm (19.5-21in) with an average of 50cm (Filipino standards po ito, pag kay Pilliteri nyo tinignan, 53cm for female and 54cm for male)
7. Growth and development in a child progresses in the following ways EXCEPT
a. From cognitive to psychosexual
b. From trunk to the tip of the extremities
c. From head to toe
d. From general to specific
Growth and development occurs in cephalo-caudal (head to toe), proximo-distal (trunk to tips of the extremities and general to specific, but it doesn’t occurs in cognitive to psychosexual because they can develop at the same time.
8. As described by Erikson, the major psychosexual conflict of the above situation is
a. Autonomy vs. Shame and doubt
b. Industry vs. Inferiority
c. Trust vs. mistrust
d. Initiation vs. guilt
According to Erikson, children 0-18 months are under the developmental task of Trust vs. Mistrust.
9. Which of the following is true about Mongolian Spots?
a. Disappears in about a year
b. Are linked to pathologic conditions
c. Are managed by tropical steroids
d. Are indicative of parental abuse
Mongolian spots are stale grey or bluish patches of discoloration commonly seen across the sacrum or buttocks due to accumulation of melanocytes and they disappears in 1 year. They are not linked to steroid use and pathologic conditions.
10. Signs of cold stress that the nurse must be alert when caring for a Newborn is:
a. Hypothermia
b. Decreased activity level
c. Shaking
d. Increased RR
Correct answer is letter D. Hypothermia is inaccurate cause normally, temperature of a newborn drop, Also a child under cold stress will kick and cry to increase the metabolic rate thereby increasing heat so B isn’t a good choice. A newborn doesn’t have the ability to shiver (Pag ikaw ay nag pa anak at ang beybe ay nanga-ngatog, naku itapon mo yan..di yan beybe itik yan.. hehe). So letter B and C is wrong. A newborn will increase its RR because the NB will need more oxygen because of too much activity.
Situation 3 Nursing care after delivery has an important aspect in every stages of delivery
11. After the baby is delivered, the cord was cut between two clamps using a sterile scissors and blade, then the baby is placed at the:
a. Mother’s breast
b. Mother’s side
c. Give it to the grandmother
d. Baby’s own mat or bed
Of course, place it at the mother’s breast for latch-on. (Note: for NSD breast feed ASAP while for CS delivery, breast feed after 4 hours) Lol, syempre d naman pwede sa grandma dba? Kasi naman hindi gatas ang ipapadede nyan, yogurt na sosyal. ewwww. LOL
12. The baby’s mother is RH(-). Which of the following laboratory tests will probably be ordered for the newborn?
a. Direct Coomb’s
b. Indirect Coomb’s
c. Blood culture
d. Platelet count
Coomb’s test is the test to determine if RH antibodies are present. Indirect Coomb’s is done to the mother and Direct Coomb’s is the one don’t to the baby. Blood culture and Platelet count doesn’t help detect RH antibodies.
13. Hypothermia is common in newborn because of their inability to control heat. The following would be an appropriate nursing intervention to prevent heat loss except
a. Place the crib beside the wall
b. Doing Kangaroo care
c. By using mechanical pressure
d. Drying and wrapping the baby
Placing the crib beside the wall is un-appropriate because it can provide heat loss by radiation. Doing Kangaroo care or hugging the baby, mechanical pressure or incubators and drying and wrapping the baby will help conserve heat,
14. The following conditions are caused by cold stress except
a. Hypoglycemia
b. Increase ICP
c. Metabolic acidosis
d. Cerebral palsy
Hypoglycemia may occur due to increase metabolic rate, And because of newborns are born slightly acidic, and they catabolize brownfat which will produce ketones which is an acid will cause metabolic acidosis. Also a NB with severe hypothermia is in high risk for kernicterus (too much bilirubin in the brain) can lead to Cerebral palsy. There is no connection in the increase of ICP with hypothermia.
(NOTE: pathognomonic sign of Kernicterus in adult- asterexis, or involuntary flapping of the hand.)
15. During the feto-placental circulation, the shunt between two atria is called
a. Ductus venosous
b. Foramen Magnum
c. Ductus arteriosus
d. Foramen Ovale
Foramen ovale is opening between two atria, Ductus venosus is the shunt from liver to the inferior vena cava, and your Ductus Arteriosus is the shunt from the pulmonary artery to the aorta. (hindi kasali sa feto-placental circulation ang Foramen Magnum, sa skull un!)
16. What would cause the closure of the Foramen ovale after the baby had been delivered?
a. Decreased blood flow
b. Shifting of pressures from right side to the left side of the heart
c. Increased PO2
d. Increased in oxygen saturation
During feto-placental circulation, the pressure in the heart is much higher in the right side, but once breathing/crying is established, the pressure will shift from the R to the L side, and will facilitate the closure of Foramen Ovale. (Note: that is why you should position the NB in R side lying position to increase pressure in the L side of the heart.)
Review:
Increase PO2-> closure of ductus arteriosus
Decreased bloodflow -> closure of the ductus venosus
Circulation in the lungs is initiated by -> lung expansion and pulmonary ventilation
What will sustain 1st breath-> decreased artery pressure
What will complete circulation-> cutting of the cord
17. Failure of the Foramen Ovale to close will cause what Congenital Heart Disease?
a. Total anomalous Pulmunary Artery
b. Atrial Septal defect
c. Transposition of great arteries
d. Pulmunary Stenosis
Foramen ovale is the opening between two Atria so, if its will not close Atrial Septal defect can occur.
Situation 4 Children are vulnerable to some minor health problems or injuries hence the nurse should be able to teach mothers to give appropriate home care.
18. A mother brought her child to the clinic with nose bleeding. The nurse showed the mother the most appropriate position for the child which is:
a. Sitting up
b. With low back rest
c. With moderate back rest
d. Lying semi flat
The correct position is making the child having an upright sitting position with the head slightly tilted forward. This position will minimize the amount of blood pressure in nasal vessels and keep blood moving forward not back into the nasopharynx, which will have the choking sensation and increase risk of aspiration. Choices b, c, d, are inappropriate cause they can cause blood to enter the nasopharynx.
19. A common problem in children is the inflammation of the middle ear. This is related to the malfunctioning of the:
a. Tympanic membrane
b. Eustachian tube
c. Adenoid
d. Nasopharynx
This is because children has short, horizontal Eustachian tubes. The dysfunction in the Eustachian tube enables bacterial invasion of the middle ear and obstructs drainage of secretions.
20. For acute otitis media, the treatment is prompt antibiotic therapy. Delayed treatment may result in complications of:
a. Tonsillitis
b. Eardrum Problems
c. Brain damage
d. Diabetes mellitus
One of the complication of recurring acute otitis media is risk for having Meningitis, thereby causing possible brain damage. That is why patient must follow a complete treatment regimen and follow up care. A and B are not complications of AOM, (lalo na ung D!!)
21. When assessing gross motor development in a 3 year old, which of the following activities would the nurse expect to finds?
a. Riding a tricycle
b. Hopping on one foot
c. Catching a ball
d. Skipping on alternate foot.
Answer is A, riding a tricycle is appropriate for a 3 y/o child. Hopping on one foot can be done by a 4 y/o child, as well as catching and throwing a ball over hand. Skipping can be done by a 5 y/o.
22. When assessing the weight of a 5-month old, which of the following indicates healthy growth?
a. Doubling of birth weight
b. Tripling of birth weight
c. Quadrupling of birth weight
d. Stabilizing of birth weight
During the first 6 months of life the weight from birth will be doubled and as soon as the baby reaches 1 year, its birth weight is tripled.
23. An appropriate toy for a 4 year old child is:
a. Push-pull toys
b. Card games
c. Doctor and nurse kits
d. Books and Crafts
Letter C is appropriate because it will enhance the creativity and imagination of a pre-school child. Letter B and D are inappropriate because they are too complex for a 4 y/o. Push-pull toys are recommended for infants.
24. Which of the following statements would the nurse expects a 5-year old boy to say whose pet gerbil just died
a. “The boogieman (kamatayan- the man with the scythe) got him”
b. “He’s just a bit dead”
c. “Ill be good from now own so I wont die like my gerbil”
d. “Did you hear the joke about…”
A 5 y/o views death in “degrees”, so the child most likely will say that “he is just a bit dead”. Personification of death like boogeyman or “kamatayan” occurs in ages 7 to 9 as well as denying death can if they will be good. Denying death using jokes and attributing life qualities to death occurs during age 3-5.
25. When assessing the fluid and electrolyte balance in an infant, which of the following would be important to remember?
a. Infant can concentrate urine at an adult level
b. The metabolic rate of an infant is slower than in adults
c. Infants have more intracellular water that adult do
d. Infant have greater body surface area than adults
Infants have greater body surface area than adult, increasing their risk to F&E imbalances. Also infants cant concentrate a urine at an adult level and their metabolic rate, also called water turnover, is 2 to 3 times higher than adult. Plus more fluids of the infants are at the ECF spaces not in the ICF spaces.
26. When assessing a child with aspirin overdose, which of the following will be expected?
a. Metabolic alkalosis
b. Respiratory alkalosis
c. Metabolic acidosis
d. Respiratory acidosis
Remember that Aspirin is acid (Acetylsalicylic ACID), so what do you expect? (ang taray LOL) UN NA!
Review:
Pag galling sa bibig: alkalosis (hyper-emesis)
Pag galling sap wet: acidosis (diarrhea)
27. Which of the following is not a possible systemic clinical manifestation of severe burns?
a. Growth retardation
b. Hypermetabolism
c. Sepsis
d. Blisters and edema
The question was asking for a SYSTEMIC clinical manifestation, Letters A,B and C are systemic manifestations while Blisters and Edema weren’t.
28. When assessing a family for potential child abuse risks, the nurse would observe for which of the following?
a. Periodic exposure to stress
b. Low socio-economic status
c. High level of self esteem
d. Problematic pregnancies
Answer is D, Typical factors that may be risk for Child abuse are problematic pregnancies, chronic exposure to stress not periodic, low level of self esteem not high level. Also child abuse can happen in all socio-economic status not just on low socio-economic status.
29. Which of the following is a possible indicator of Munchausen syndrome by proxy type of child abuse?
a. Bruises found at odd locations, with different stages of healing
b. STD’s and genital discharges
c. Unexplained symptoms of diarrhea, vomiting and apnea with no organic basis
d. Constant hunger and poor hygiene
Munchausen syndrome by Proxy is the fabrication or inducement of an illness by one person to another person, usually mother to child. It is characterized by symptoms such as apnea and siezures, which may be due to suffocation, drugs or poisoning, vomiting which can be induced with poisons and diarrhea with the use of laxatives. Letter A can be seen in a Physical abuse, Letter B for sexual abuse and Letter C is for Physical Neglect.
30. Which of the following is an inappropriate intervention when caring for a child with HIV?
a. Teaching family about disease transmission
b. Offering large amount of fresh fruits and vegetables
c. Encouraging child to perform at optimal level
d. Teach proper hand washing technique
A child with HIV is immunocompromised. Fresh fruits and vegetables, which may be contaminated with organisms and pesticides can be harmful, if not fatal to the child, therefore these items should be avoided.
Situation 5 Agata, 2 years old is rushed to the ER due to cyanosis precipitated by crying. Her mother observed that after playing she gets tired. She was diagnosed with Tetralogy of Fallot.
31. The goal of nursing care fro Agata is to:
a. Prevent infection
b. Promote normal growth and development
c. Decrease hypoxic spells
d. Hydrate adequately
The correct answer is letter C. Though letter B would be a good answer too, this goal is too vague and not specific. Nursing interventions will not solely promote normal G&D unless he will undergo surgical repair. So decreasing Hypoxic Spells is more SMART. (alam nyo na kung ano yun! Specific, measurable, attainable, realistic and time bounded). Letter A and D are inappropriate.
REVIEW! REVIEW! REVIEW!
Tetralogy of Fallot is a cyanotic Congenital Heart disease. Kaya sa tinawag na Tetralogy cause it has 4 anomalies;
1. VSD- ventricular septal defect
2. Pulmunary Stenosis
3. Over-riding of the Aorta- the aorta overrides both ventricles
4. Right ventricular hypertrophy
We have 14 congenital heart defects. 8 acyanotic and 6 cyanoyic.
8 Acyanotice includes: ASD, VSD, PDA, endocardial cushion defect, pulmonary stenosis, doupling of the aorta, Aortic stenosis and Coarctation of the Aorta
6 Cyanotic includes: Tetralogy of fallot, Total anomalous pulmonary artery, Transposition of the great arteries, Truncus arteriousus, Hypoplastic Left heart syndrome.
(Acyanotic causes L->R shunting while cyanotic cause R->L shunting. Para madaling matandaan lahat ng may “T” eh cyanotic OK?
32. The immediate nursing intervention for cyanosis of Agata is:
a. Call up the pediatrician
b. Place her in knee chest position
c. Administer oxygen inhalation
d. Transfer her to the PICU
The immediate intervention would be to place her on knee-chest or “squatting” position because it traps blood into the lower extremities. Though also letter C would be a good choice but the question is asking for “Immediate” so letter B is more appropriate. Letter A and D are incorrect because its normal for a child who have ToF to have hypoxic or “tets” spells so there is no need to transfer her to the NICU or to alert the Pediatrician.
33. Agata was scheduled for a palliative surgery, which creates anastomosis of the subclavian artery to the pulmonary artery. This procedure is:
a. Waterston-Cooley
b. Raskkind Procedure
c. Coronary artery bypass
d. Blalock-Taussig
Correct answer is Blalock-Taussig procedure its just a temporary or palliative surgery which creates a shunt between the aorta and pulmonary artery (oist parang ductus arteriosus) so that the blood can leave the aorta and enter the pulmonary artery and thus oxygenating the lungs and return to the left side of the heart, then to the aorta then to the body. This procedure also makes use of the subclavian vein so pulse is not palpable at the right arm.
The full repair for ToF is called the Brock procedure. Raskkind is a palliative surgery for TOGA.
34. Which of the following is not an indicator that Agata experiences separation anxiety brought about her hospitalization?
a. Friendly with the nurse
b. Prolonged loud crying, consoled only by mother
c. Occasional temper tantrums and always says NO
d. Repeatedly verbalizes desire to go home
Because toddlers views hospitalization is abandonment, separation anxiety is common. Its has 3 phases: PDD (parang c puff daddy LOL)
1. Protest 2. despair 3. detachment (or denial). Choices B, C, D are usually seen in a child with separation anxiety (usually in the protest stage).
REVIEW:
Separation anxiety begin at: 9 months
Peaks: 18 months
35. When Agata was brought to the OR, her parents where crying. What would be the most appropriate nursing diagnosis?
a. Infective family coping r/t situational crisis
b. Anxiety r/t powerlessness
c. Fear r/t uncertain prognosis
d. Anticipatory grieving r/t gravity of child’s physical status
In this item letter A and be are inappropriate response so remove them. The possible answers are C and D. Fear defined as the perceived threat (real or imagined) that is consciously recognized as danger (NANDA) is applicable in the situation but its defining characteristics are not applicable. Crying per se can not be a subjective cue to signify fear, and most of the symptoms of fear in NANDA are physiological. Anticipatory grieving on the other hand are intellectual and EMOTIONAL responses based on a potential loss. And remember that procedures like this cannot assure total recovery. So letter D is a more appropriate Nursing diagnosis.
NOTE: GANATO NA PO ANG PATTERN NG NLE, LAGING MAY HALONG THERAPUETIC COMMUNICATION AT NURSING DIAGNOSIS.
36. Which of the following respiratory condition is always considered a medical emergency?
a. Laryngeotracheobronchitis (LTB)
b. Epiglottitis
c. Asthma
d. Cystic Fibrosis
Correct answer is letter B, because acute and sever inflammation of the epiglottis can cause life threatening airway obstruction, that is why its always treated as a medical emergency. NSG intervention : Prepare tracheostomy set at bed side.
LTB, can also cause airway obstruction but its not an emergency. Asthma is also not an emergency (ung status asthmaticus ang kaylangan ng prompt treatment). CF is a chronic disease, so its not a medical emergency.
REVIEW: Medical emergency of GI: peritonitis
37. Which of the following statements by the family of a child with asthma indicates a need for additional teaching?
a. “We need to identify what things triggers his attacks”
b. “He is to use bronchodilator inhaler before steroid inhaler”
c. “We’ll make sure he avoids exercise to prevent asthma attacks”
d. “he should increase his fluid intake regularly to thin secretions”
Asthmatic children don’t have to avoid exercise. They can participate on physical activities as tolerated. Using a bronchodilator before administering steroids is correct because steroids are just anti-inflammatory and they don’t have effects on the dilation of the bronchioles. OF course letters A and B are obviously correct.
38. Which of the following would require careful monitoring in the child with ADHD who is receiving Methylphenidate (Ritalin)?
a. Dental health
b. Mouth dryness
c. Height and weight
d. Excessive appetite
Dental problems are more likely to occur in children under going TCA therapy. Mouth dryness is a expected side effects of Ritalin since it activates the SNS. Also loss of appetite is more likely to happen, not increase in appetite. The correct answer is letter C, because Ritalin can affect the child’s G&D. Intervention: medication “holidays or vacation”. (This means na.. during weekends or holidays or school vacations, where the child wont be in school, the drug can be withheld.)
Situation 6 Laura is assigned as the Team Leader during the immunization day at the RHU
39. What program for the DOH is launched at 1976 in cooperation with WHO and UNICEF to reduce morbidity and mortality among infants caused by immunizable disease?
a. Patak day
b. Immunization day on Wednesday
c. Expanded program on immunization
d. Bakuna ng kabtaan
SUS me! Dapat pa bang I-rationalize? Ang di nakakuha ng tamang sagot… hala… JOKE.. hehehe
40. One important principle of the immunization program is based on?
a. Statistical occurrence
b. Epidemiologic situation
c. Cold chain management
d. Surveillance study
Letters A, C and D are not included in the principles of EPI.
The principle of EPI are the following:
1. Its is based on epidemiological situation
2. Mass approach utilization- the whole community is to be protected rather than the individual
3. Immunization is a basic health service, and should be provided by the RHU
41. The main element of immunization program is one of the following?
a. Information, education and communication
b. Assessment and evaluation of the program
c. Research studies
d. Target setting
Correct answer is D.
The following are the elements of EPI:
• Target seting
• Cold chain logistic management
• Information, education and communication
• Assessment and evaluation of the program’s over all performance
• Surveillance, studies and research
42. What does herd immunity means?
a. Interruption of transmission
b. All to be vaccinated
c. Selected group for vaccination
d. Shorter incubation
43. Measles vaccine can be given simultaneously. What is the combined vaccine to be given to children starting at 15 months?
a. MCG
b. MMR
c. BCG
d. BBR
MMR or Measles, Mumps, Rubella is a vaccine furnished in one vial and is routinely given in one injection (Sub-Q). It can be given at 15 months but can also be given as early as 12th month.
Situation 7: Braguda brought her 5-month old daughter in the nearest RHU because her baby sleeps most of the time, with decreased appetite, has colds and fever for more than a week. The physician diagnosed pneumonia.
44. Based on this data given by Braguda, you can classify Braguda’s daughter to have:
a. Pneumonia: cough and colds
b. Severe pneumonia
c. Very severe pneumonia
d. Pneumonia moderate
For a child aging 2months up to 5 years old can be classified to have sever pneumonia when he have any of the following danger signs:
• Not able to drink
• Convulsions
• Abnormally sleepy or difficult to wake
• Stridor in calm child or
• Severe under-nutrition
45. For a 3-month old child to be classified to have Pneumonia (not severe), you would expect to find RR of:
a. 60 bpm
b. 40 bpm
c. 70 bpm
d. 50 pbm
Correct answer is letter D. A child can be classified to have Pneumonia (not severe) if:
• the young infant is less than 2 months- 60 bpm or more
• if the child is 2 months up to less than 12 months- 50 bpm or more
• if the child is 12 months to 4 y/o- 40 bpm or more
46. You asked Braguda if her baby received all vaccines under EPI. What legal basis is used in implementing the UN’s goal on Universal Child Immunization?
a. PD no. 996
b. PD no. 6
c. PD no. 46
d. RA 9173
Correct answer is letter B. Presidential Proclamation no. 6 (April 3, 1986) is the “Implementing a United Nations goal on Universal Child Immunization by 1990”. PD 996 (September 16, 1976) is “providing for compulsory basic immunization for infants and children below 8 years of age. PD no. 46 (September 16, 1992) is the “Reaffirming the commitment of the Philippines to the universal Child and Mother goal of the World Health Assembly. RA 9173 is of course the “Nursing act of 2002”
47. Braguda asks you about Vitamin A supplementation. You responded that giving Vitamin A starts when the infant reaches 6 months and the first dose is”
a. 200,000 “IU”
b. 100,000 “IU”
c. 500,000 “IU”
d. 10,000 “IU”
An infant aging 6-11 months will be given Vitamin supplementation of 100, 000 IU and for Preschoolers ages 12-83 months 200,000 “IU” will be given.
48. As part of CARI program, assessment of the child is your main responsibility. You could ask the following question to the mother except:
a. “How old is the child?”
b. “IS the child coughing? For how long?”
c. “Did the child have chest indrawing?”
d. “Did the child have fever? For how long?”
The CARI program of the DOH includes the “ASK” and “LOOK, LISTEN” as part of the assessment of the child who has suspected Pneumonia. Choices A, B and D are included in the “ASK” assessment while Chest indrawings is included in the “LOOK, LISTEN” and should not be asked to the mother.
49. A newborn’s failure to pass meconium within 24 hours after birth may indicate which of the following?
a. Aganglionic Mega colon
b. Celiac disease
c. Intussusception
d. Abdominal wall defect
Failure to pass meconium of Newborn during the first 24 hours of life may indicate Hirschsprung disease or Congenital Aganglionic Megacolon, an anomaly resulting in mechanical obstruction due to inadequate motility in an intestinal segment. B, C, and D are not associated in the failure to pass meconium of the newborn.
50. The nurse understands that a good snack for a 2 year old with a diagnosis of acute asthma would be:
a. Grapes
b. Apple slices
c. A glass of milk
d. A glass of cola
Correct answer is B, apple slices. Grapes is in appropriate because of its “balat” that can cause choking. A glass of milk is not a good snack because it’s the most common cause of Iron-deficiency anemia in children (milk contains few iron), A glass of cola is also not appropriate cause it contains complex sugar. (walang kinalaman ang asthma dahil ala naman itong diatery restricted foods na nasa choices.)
51. Which of the following immunizations would the nurse expect to administer to a child who is HIV (+) and severely immunocomromised?
a. Varicella
b. Rotavirus
c. MMR
d. IPV
IPV or Inactivated polio vaccine does not contain live micro organisms which can be harmful to an immunocompromised child. Unlike OPV, IPV is administered via IM route.
52. When assessing a newborn for developmental dysplasia of the hip, the nurse would expect to assess which of the following/
a. Symmetrical gluteal folds
b. Trendelemburg sign
c. Ortolani’s sign
d. Characteristic limp
Correct answer is Ortolani’s sign; it is the abnormal clicking sound when the hips are abducted. The sound is produced when the femoral head enters the acetabulum. Letter A is wrong because its should be “asymmetrical gluteal fold”. Letter B and C are not applicable for newborns because they are seen in older children.
53. While assessing a male neonate whose mother desires him to be circumcised, the nurse observes that the neonate’s urinary meatus appears to be located on the ventral surface of the penis. The physician is notified because the nurse would suspect which of the following?
a. Phimosis
b. Hydrocele
c. Epispadias
d. Hypospadias
Hypospadias is a c condition in which the urethral opening is located below the glans penis or anywhere along the ventral surface of the penile shaft. Epispadias, the urethral meatus is located at the dorsal surface of the penile shaft. (Para di ka malilto, I-alphabetesize mo Dorsal, (Above) eh mauuna sa Ventral (Below) , Epis mauuna sa Hypo.)
54. When teaching a group of parents about seat belt use, when would the nurse state that the child be safely restrained in a regular automobile seatbelt?
a. 30 lb and 30 in
b. 35 lb and 3 y/o
c. 40 lb and 40 in
d. 60 lb and 6 y/o
Basta tandaan ang rule of 4! 4 years old, 40 lbs and 40 in.
55. When assessing a newborn with cleft lip, the nurse would be alert which of the following will most likely be compromised?
a. Sucking ability
b. Respiratory status
c. Locomotion
d. GI function
Because of the defect, the child will be unable to form the mouth adequately arounf the nipple thereby requiring special devices to allow feeding and sucking gratification. Respiratory status may be compromised when the child is fed improperly or during post op period.
REVIEW!
Repair of cleft lip-cheiloplasty-should be done within 1-3 months- to save sucking reflex- position post-op side lying
Repair of cleft palate- Uranoplasty- should be done within 4-6 months-to preserve speech- position post-op is prone.
56. For a child with recurring nephritic syndrome, which of the following areas of potential disturbances should be a prime consideration when planning ongoing nursing care?
a. Muscle coordination
b. Sexual maturation
c. Intellectual development
d. Body image
Because of edema, associated with nephroitic syndrome, potential self concept and body image disturbance related to changes in appearance and social isolation should be considered.
HEY! NARARAMDAMAN KO NA LALABAS ULIT ANG MGA SAKIT RELATED SA NEW BORN SCREENING KAYA ARALIN NA ITO. I WILL POST A SIMPLE LECTURE DITO. (LATER…. Kasi tamad ako,,, hehehe)
57. An inborn error of metabolism that causes premature destruction of RBC?
a. G6PD
b. Hemocystinuria
c. Phenylketonuria
d. Celiac Disease
G6PD is the premature destruction of RBC when the blood is exposed to antioxidants, ASA (ano un? Aspirin), legumes and flava beans.
58. Which of the following would be a diagnostic test for Phenylketonuria which uses fresh urine mixed with ferric chloride?
a. Guthrie Test
b. Phenestix test
c. Beutler’s test
d. Coomb’s test
Phenestix test is a diagnostic test which uses a fresh urine sample (diapers) and mixed with ferric chloride. If positive, there will be a presence of green spots at the diapers. Guthrie test is another test for PKU and is the one that mostly used. The specimen used is the blood and it tests if CHON is converted to amino acid.
59. Dietary restriction in a child who has Hemocystenuria will include which of the following amino acid?
a. Lysine
b. Methionine
c. Isolensine tryptophase
d. Valine
Hemocystenuria is the elevated excretion of the amino acid hemocystiene, and there is inability to convert the amino acid methionine or cystiene. So dietary restriction of this amino acids is advised. This disease can lead to mental retardation.
60. A milk formula that you can suggest for a child with Galactosemia:
a. Lofenalac
b. Lactum
c. Neutramigen
d. Sustagen
Neutramigen is suggested for a child with Galactosemia. Lofenalac is suggested for a child with PKU. Sustagen is for Susy and Geno, Lactum.. lactum..
MEDICAL SURGICAL NURSING
SITUATION : Dervid, A registered nurse, witnessed an old woman hit by a motorcycle while crossing a train railway. The old woman fell at the railway. Dervid Rushed at the scene.
1. As a registered nurse, Dervid knew that the first thing that he will do at the scene is [3]
A. Stay with the person, Encourage her to remain still and Immobilize the leg while
While waiting for the ambulance.
B. Leave the person for a few moments to call for help.
C. Reduce the fracture manually.
D. Move the person to a safer place.
* The old woman is in the middle of a train railway. It is very unsafe to immobilize here legs and remain still at the middle of a railway considering that a train might come anytime while waiting for an ambulance. Safety is the utmost importance at this point. If letter D is not among the choices and the situation is a little less dangerous, the answer will be A. Remember that in all cases of emergencies, removing the victim from the scene to a much safer place is a priority.
2. Dervid suspects a hip fracture when he noticed that the old woman’s leg is [4]
A. Lengthened, Abducted and Internally Rotated.
B. Shortened, Abducted and Externally Rotated.
C. Shortened, Adducted and Internally Rotated.
D. Shortened, Adducted and Externally Rotated.
* SADDER should be your keyword. A hip fracture will produce a SHORTENED, ADDUCTED AND EXTERNALLY ROTATED extremity. Treatment will evolve in casting the leg and putting it in a EXTENSION, NEUTRALLY POSITIONED and SLIGHT INTERNAL ROTATION. In Hip prosthesis, The nurse should maintain the client’s leg in FLEXION, EXTERNAL ROTATION and ABDUCTION to prevent the dislocation of the prosthesis from the acetabulum. Take note of the difference because I mistakenly answered the LATTER in casting a hip fracture thinking that it is similar to a the leg positioning in hip dislocation. Just imagine a patient with a cast that has his leg in ABDUCTION, EXTERNAL ROTATION AND FLEXION. It will cause flexion contractures.
3. The old woman complains of pain. John noticed that the knee is reddened, warm to touch and swollen. John interprets that this signs and symptoms are likely related to [2]
A. Infection
C. Thrombophlebitis
B. Inflammation
D. Degenerative disease
* After a trauma, Inflammation will start almost instantly. Infection occurse 24-48 hours after bone fracture and not immediately. Thrombophlebitis occurs within 4 to 7 days of hospitalization after prolonged immobilization. There is no evidence that the client has a degenerative disease and degenerative diseases will manifest in variety of ways and not after a trauma.
4. The old woman told John that she has osteoporosis; Dervid knew that all of the following factors would contribute to osteoporosis except [4]
A. Hypothyroidism
B. End stage renal disease
C. Cushing’s Disease
D. Taking Furosemide and Phenytoin.
* B,C,D all contributes to bone deminiralization except HYPOTHYROIDISM. Hyperthyroidism will contribute to bone deminiralization as well as Hyperparathyroidism due to the increase in PTH, It will cause the movement of calcium from the bone to the blood causing HYPERCALCEMIA. ESRD will cause increase in PHOPHSATE due to its poor excretion. The amount of phosphate is inversely proportional to the amount of calcium. Cushing disease promotes bone demineralization as well as medications like diuretics and anti convulsants.
5. Martha, The old woman was now Immobilized and brought to the emergency room. The X-ray shows a fractured femur and pelvis. The ER Nurse would carefully monitor Martha for which of the following sign and symptoms? [3]
A. Tachycardia and Hypotension
B. Fever and Bradycardia
C. Bradycardia and Hypertension
D. Fever and Hypertension
* hemorrhage results in severing of the vascular supply of the bone of the femur and the pelvis due to the fracture leading to bleeding causing the s/s of tachycardia and hypotension.
SITUATION: Mr. D. Rojas, An obese 35 year old MS Professor of OLFU Lagro is admitted due to pain in his weight bearing joint. The diagnosis was Osteoarthritis.
6. As a nurse, you instructed Mr. Rojas how to use a cane. Mr. Rojas has a weakness on his right leg due to self immobilization and guarding. You plan to teach Mr. Rojas to hold the cane [4]
A. On his left hand, because his right side is weak.
B. On his left hand, because of reciprocal motion.
C. On his right hand, to support the right leg.
D. On his right hand, because only his right leg is weak.
* Reciprocal motion is a very important aspect of rehabilitation. Mr. Rojas has a weakness on his right leg. If a human moves his right leg, the left arm will accompany the movement of the right leg. That is what you call RECIPROCAL MOTION which is innate, natural and required to maintain balance. Mr. Rojas has weakness in his RIGHT LEG. If we put the cane on his right arm, The client will then be left UNSUPPORTED when he use his stronger leg [LEFT LEG] and stand with his weaker leg [RIGHT LEG] due to the fact that the opposite arm must accompany the movement of the opposite leg [RIGHT ARM]. In a more easier term, Always put the cane on the opposite of the weaker side. A is not correct because the client is NOT hemiplegic and will never be correct to reason out why the cane must always be at the opposite of the weaker side, it will always be due to reciprocal motion.
7. You also told Mr. Rojas to hold the cane [4]
A. 1 Inches in front of the foot.
B. 3 Inches at the lateral side of the foot.
c. 6 Inches at the lateral side of the foot.
D. 12 Inches at the lateral side of the foot.
* Remove option A, the client will kick off the cane if it was in the front of the foot. Remove option D because that is too far and will cause the cane to poorly support the client because the side, not the tip, is touching the ground. At 3 inches, imagine how short it is and will cause a very poor supporting base. The correct answer is anywhere from 6 to 10 inches for both crutches and cane.
8. Mr. Rojas was discharged and 6 months later, he came back to the emergency room of the hospital because he suffered a mild stroke. The right side of the brain was affected. At the rehabilitative phase of your nursing care, you observe Mr. Rojas use a cane and you intervene if you see him [4]
A. Moves the cane when the right leg is moved.
B. Leans on the cane when the right leg swings through.
C. keeps the cane 6 Inches out to the side of the right foot.
D. Holds the cane on the right side.
* If the right side of the brain is affected, weakness will always be CONTRALATERAL and therefore, Mr. Rojas will have weakness on his left side. Earlier I told you that cane is held on the opposite side of the weaker side, which in this situation, will be on the RIGHT. Imagine if the client moves his RIGHT LEG together witht the RIGHT CANE, it already violated the LAW OF RECIPROCAL MOTION. Moving the right leg will require Mr. Rojas to move his left arm and not the cane, which is on his right.
SITUATION: Alfred, a 40 year old construction worker developed cough, night sweats and fever. He was brought to the nursing unit for diagnostic studies. He told the nurse he did not receive a BCG vaccine during childhood
9. The nurse performs a Mantoux Test. The nurse knows that Mantoux Test is also known as [1]
A. PPD
B. PDP
C. PDD
D. DPP
* PPD stands for purified protein derivative. It is used to check for TB exposure. All clients who had BCG need not perform this test because they will always be + .
10. The nurse would inject the solution in what route? [1]
A. IM
B. IV
C. ID
D. SC
* A Wheal is created intradermally and then it is marked and timed. reading will be done within 2 to 3 days.
11. The nurse notes that a positive result for Alfred is [2]
A. 5 mm wheal
B. 5 mm Induration
C. 10 mm Wheal
D. 10 mm Induration
* 10 mm Induration [ redness ] is considered positive for individuals with competitive immune response. Wheals are not measured, they will not anymore enlarge. A 5 mm induration is considered positive for patients with AIDS or immunocompromised.
12. The nurse told Alfred to come back after [2]
A. a week
B. 48 hours
C. 1 day
D. 4 days
* Clients are asked to comeback within 2 to 3 days for the reading.
13. Mang Alfred returns after the Mantoux Test. The test result read POSITIVE. What should be the nurse’s next action? [3]
A. Call the Physician
B. Notify the radiology dept. for CXR evaluation
C. Isolate the patient
D. Order for a sputum exam
* The nurse has no authority order the radiology department for a chest x ray evaluation nor order for a sputum exam. The client need not be isolated because Mantoux test do not determine the activeness of the disease.
14. Why is Mantoux test not routinely done in the Philippines? [2]
A. It requires a highly skilled nurse to perform a Mantoux test
B. The sputum culture is the gold standard of PTB Diagnosis and it will definitively determine the extent of the cavitary lesions
C. Chest X Ray Can diagnose the specific microorganism responsible for the lesions
D. Almost all Filipinos will test positive for Mantoux Test
* almost all filipinos tests positive for mantoux test due to the fact that BCG are required and TB exposure in the country is fullminant. All individuals vaccinated with BCG will test POSITIVE for mantoux test all their lives.
15. Mang Alfred is now a new TB patient with an active disease. What is his category according to the DOH? [1]
A. I
B. II
C. III
D. IV
* Category I patients are those with a newly diagnosed TB whose sputum culture are positive. II are for those who have relapses while III are those with negative sputum culture but positive chest x ray, or PTB Minimal.
16. How long is the duration of the maintenance phase of his treatment? [2]
A. 2 months
B. 3 months
C. 4 months
D. 5 months
* Clients in category I will have 2 months INTENSIVE and 4 months maintenance treatment.
17. Which of the following drugs is UNLIKELY given to Mang Alfred during the maintenance phase? [3]
A. Rifampicin
B. Isoniazid
C. Ethambutol
D. Pyridoxine
* Drugs given in the maintenance phase includes Rifampicin and Isoniazid. Ethambutol is given on the intensive phase along with rifampicin and isoniazid. Pyridoxine is given during Isoniazid treatment to prevent peripheral neuritis in contrast in treatment of parkinson's with levodopa, Pyridoxine or VB6 is restricted.
18. According to the DOH, the most hazardous period for development of clinical disease is during the first [4]
A. 6-12 months after
B. 3-6 months after
C. 1-2 months after
D. 2-4 weeks after
* According to the department of health, the most hazardous period for development of clinical disease is during the first 6 to 12 months.
19. This is the name of the program of the DOH to control TB in the country [2]
A. DOTS
B. National Tuberculosis Control Program
C. Short Coursed Chemotherapy
D. Expanded Program for Immunization
* National tuberculosis control program is the name of the program of the DOH to control and eradicate TB in the country. DOTS refers to the STRATEGY used by the department in treating TB patients. EPI is not a program for TB control although BCG is one of the vaccine given in this program.
20. Susceptibility for the disease [ TB ] is increased markedly in those with the following condition except [3]
A. 23 Year old athlete with diabetes insipidus
B. 23 Year old athlete taking long term Decadron therapy and anabolic steroids
C. 23 Year old athlete taking illegal drugs and abusing substances
D. Undernourished and Underweight individual who undergone gastrectomy
* Nutrition, Long term immunosupression and drug abuse are all factors that affects the resistance of an individual in acquiring communicable diseases. Other factors includes extremes of ages, poor environmental sanitation, poverty and poor living conditions. Diabetes insipidus does not, in anyway alter a persons immune response.
21. Direct sputum examination and Chest X ray of TB symptomatic is in what level of prevention? [1]
A. Primary
B. Secondary
C. Tertiary
D. Quarterly
* National board exam loves asking about level of prevention. Mastery with the primary, secondary and tertiary levels of prevention is a must. All diagnostic, case finding and treatment belongs to the secondary level of prevention.
SITUATION: Michiel, A male patient diagnosed with colon cancer was newly put in colostomy.
22. Michiel shows the BEST adaptation with the new colostomy if he shows which of the following? [2]
A. Look at the ostomy site
B. Participate with the nurse in his daily ostomy care
C. Ask for leaflets and contact numbers of ostomy support groups
D. Talk about his ostomy openly to the nurse and friends
* Actual participation conveys positive acceptance and adjustment to the altered body image. Although looking at the ostomy site also conveys acceptance and adjustment, Participating with the nurse to his daily ostomy care is the BEST adaptation a client can make during the first few days after colostomy creation.
23. The nurse plans to teach Michiel about colostomy irrigation. As the nurse prepares the materials needed, which of the following item indicates that the nurse needs further instruction? [3]
A. Plain NSS / Normal Saline
B. K-Y Jelly
C. Tap water
D. Irrigation sleeve
* The colon is not sterile, nor the stomach. Tap water is used in enema irrigation and not NSS. Although some clients would prefer a distilled, mineral or filtered water, NSS is not always necessary. KY Jelly is used as the lubricant for the irrigation tube and is inserted 3-4 inches into the colostomy pointing towards the RIGHT. Irrigation sleeve is use to direct the flow of the irrigated solution out of the stomach and into the bedpan or toilet.
24. The nurse should insert the colostomy tube for irrigation at approximately [3]
A. 1-2 inches
B. 3-4 inches
C. 6-8 inches
D. 12-18 inches
* Remember 3-4 inches. They are both used in the rectal tube and colostomy irrigation tube insertion. 1 to 2 inches is too short and may spill out the irrigant out of the stoma. Starting from 6 inches, it would be too long already and may perforate the bowel.
25. The maximum height of irrigation solution for colostomy is [3]
A. 5 inches
B. 12 inches
C. 18 inches
D. 24 inches
* If you will answer in the CGFNS and NCLEX, C will be the correct answer. According to BRUNNER AND SUDDARTHS and Saunders, The height of the colostomy irrigation bag should be hanging above the clients shoulder at around 18 inches. According to MOSBY, 12 inches should be the maximum height. According to Lippinncots, 18 inches is the maximum height. According the the board of examiners, 12 inches should be the maximum height and an 18 inches irrigant height would cause rapid flow of the irrigant towards the colostomy. Therefore, answer in the local board should only be at 12 inches.
26. Which of the following behavior of the client indicates the best initial step in learning to care for his colostomy? [1]
A. Ask to defer colostomy care to another individual
B. Promises he will begin to listen the next day
C. Agrees to look at the colostomy
D. States that colostomy care is the function of the nurse while he is in the hospital
* The client made the best initial step in learning to care for his colostomy once he looks at the site. This is the start of the client's acceptance on his altered body image. A,B and D delays learning and shows the client's disintrest regarding colostomy care.
27. While irrigating the client’s colostomy, Michiel suddenly complains of severe cramping. Initially, the nurse would [1]
A. Stop the irrigation by clamping the tube
B. Slow down the irrigation
C. Tell the client that cramping will subside and is normal
D. Notify the physician
* Stopping the irrigation will also stop the cramping and pain. During the first few days of irrigation, The client will feel pain and cramping as soon as the irirgant touches the bowel. This will start to lessen once the client got accustomed to colostomy irrigation. Slowing down the irrigation will not stop the pain. Telling the client that it is normal and will subside eventually is not acceptable when a client experiences pain. Pain is all encompasing and always a priority over anything else in most situations. Notifying the physician will not be helpful and unecessary.
28. The next day, the nurse will assess Michiel’s stoma. The nurse noticed that a prolapsed stoma is evident if she sees which of the following? [1]
A. A sunken and hidden stoma
B. A dusky and bluish stoma
C. A narrow and flattened stoma
D. Protruding stoma with swollen appearance
* A refers to a retracted stoma, B refers to a stoma that is getting a very poor blood supply. C is a description of stenosis of the stoma.
29. Michiel asked the nurse, what foods will help lessen the odor of his colostomy. The nurse best response would be [4]
A. Eat eggs
B. Eat cucumbers
C. Eat beet greens and parsley
D. Eat broccoli and spinach
* Kinchay and Pechay helps lessen the odor of the colostomy. Spinach, broccoli, Cabbage, Cucumbers, Patola or bottle gourd also help lessen the odor BUT are gas formers. Eggs are not recommended because they are known to cause unpleasant odors in patients with colostomy.
30. The nurse will start to teach Michiel about the techniques for colostomy irrigation. Which of the following should be included in the nurse’s teaching plan? [4]
A. Use 500 ml to 1,000 ml NSS
B. Suspend the irrigant 45 cm above the stoma
C. Insert the cone 4 cm in the stoma
D. If cramping occurs, slow the irrigation
* 1 inches is equal to 2.54 cm. Convert the cm if you are not familiar. 45 cm is around 17 inches which is ideal for colostomy irrigation. Any value from 12 to 18 is accepted as the colostomy irrigant height. Tap water is used as an irrigant and is infused at room temperature. 4 cm is a little bit short for the ideal 3-4 inches. If cramping occurs STOP the irrigation and continue when is subsides.
31. The nurse knew that the normal color of Michiel’s stoma should be [1]
A. Brick Red
B. Gray
C. Blue
D. Pale Pink
* The stoma should be RED in color. Pale pink are common with anemic or dehydrated patients who lost a lot of blood after an operation. Blue stoma indicated cyanosis or alteration in perfusion. Stomas are not expected to be Gray.
SITUATION: James, A 27 basketball player sustained inhalation burn that required him to have tracheostomy due to massive upper airway edema.
32. Wilma, His sister and a nurse is suctioning the tracheostomy tube of James. Which of the following, if made by Wilma indicates that she is committing an error? [2]
A. Hyperventilating James with 100% oxygen before and after suctioning
B. Instilling 3 to 5 ml normal saline to loosen up secretion
C. Applying suction during catheter withdrawal
D. Suction the client every hour
* This is unecessary. Suctioning is done on PRN basis and not every hour. A,B and C are all correct processes of suctioning a tracheostomy.
33. What size of suction catheter would Wilma use for James, who is 6 feet 5 inches in height and weighing approximately 145 lbs? [2]
A. Fr. 5
B. Fr. 10
C. Fr. 12
D. Fr. 18
* The height is given and it looks like james is a very tall individual. The maximum height of suction tube is used. fr 12-18 are used for adults while 6-8 are used in children.
34. Wilma is using a portable suction unit at home, What is the amount of suction required by James using this unit? [4]
A. 2-5 mmHg
B. 5-10 mmHg
C. 10-15 mmHg
D. 20-25 mmHg
* A is used in pediatric clients. B is for children and C is for adults. 20-25 mmHg is too much for a portable suction unit and is not recommended.
35. If a Wall unit is used, What should be the suctioning pressure required by James? [4]
A. 50-95 mmHg
B. 95-110 mmHg
C. 100-120 mmHg
D. 155-175 mmHg
* A is used in pediatric clients. B is for children and C is for adults. 155-175 mmHg is too much for a wall suction unit and is not recommended.
36. Wilma was shocked to see that the Tracheostomy was dislodged. Both the inner and outer cannulas was removed and left hanging on James’ neck. What are the 2 equipment’s at james’ bedside that could help Wilma deal with this situation? [3]
A. New set of tracheostomy tubes and Oxygen tank
B. Theophylline and Epinephrine
C. Obturator and Kelly clamp
D. Sterile saline dressing
* In an emergency like this, The first thing the nurse should do is maintaining the airway patency. With the cannunlas dislodged, The stoma will stenosed and narrows giving james an obstructed airway. The nurse would insert the kelly clamp to open the stoma and lock the clamp in place to maintain it open while she uses an obturator as to prevent further stenosis of the stoma. An obturator is a part of the NGT package included by most manufacturers to guide the physician or nurses in inserting the outer cannula.
37. Which of the following method if used by Wilma will best assure that the tracheostomy ties are not too tightly placed? [2]
A. Wilma places 2 fingers between the tie and neck
B. The tracheotomy can be pulled slightly away from the neck
C. James’ neck veins are not engorged
D. Wilma measures the tie from the nose to the tip of the earlobe and to the xiphoid process.
* Wilma should place 2 fingers underneath the tie to ensure that it is not too tight nor too loose. Letter D is the measurement for NGT insertion and is unrelated to tracheostomy.
38. Wilma knew that James have an adequate respiratory condition if she notices that [1]
A. James’ respiratory rate is 18
B. James’ Oxygen saturation is 91%
C. There are frank blood suction from the tube
D. There are moderate amount of tracheobronchial secretions
* an RR of 18 means that James is not tachypneic and has an adequate air exchange. Oxygen saturation should be more than 95%. Frank blood is not expected in the suction tube. A slight tinged of blood in the tube is acceptable and expected. Amount of secretion are not in anyway related in assessing the respiratory condition of a person and so is the amount of blood in the tube.
39. Wilma knew that the maximum time when suctioning James is [1]
A. 10 seconds
B. 20 seconds
C. 30 seconds
D. 45 seconds
* According to our reviewers and lecturers, 10 to 15 seconds is the maximum suction time. But according to almost all foreign books I read, it should only be 10 seconds at max. I prefer following Saunders,Mosby and Lippinncots when they are all united.
SITUATION : Juan Miguel Lopez Zobel Ayala de Batumbakal was diagnosed with Acute Close Angle Glaucoma. He is being seen by Nurse Jet.
40. What specific manifestation would nurse Jet see in Acute close angle glaucoma that she would not see in an open angle glaucoma? [3]
A. Loss of peripheral vision
B. Irreversible vision loss
C. There is an increase in IOP
D. Pain
* There is NO PAIN in open angle glaucoma. A,B,C are all present in both glaucomas including the low pressure glaucoma. Pain is absent because the increase in intra ocular pressure is not initiated abruptly. It is gradual and progressive and will lead to unoticed loss of peripheral vision. Pain is present in acute close angle glaucoma because there is a sudden closure or narrowing of the canal of schlemm. Therefore if you will be ask what s/s is common in both, answer IRREVERSIBLE LOSS OF PERIPHERAL VISION.
41. Nurse jet knew that Acute close angle glaucoma is caused by [3]
A. Sudden blockage of the anterior angle by the base of the iris
B. Obstruction in trabecular meshwork
C. Gradual increase of IOP
D. An abrupt rise in IOP from 8 to 15 mmHg
* Sudden blockage of the angle will cause s/s of acute angle closure glaucoma. B and C are all related to open angle glaucoma. D is insignificant, If the client bends or cough, IOP can increase from 8 to as much as 30 mmHg but then return again to normal.
42. Nurse jet performed a TONOMETRY test to Mr. Batumbakal. What does this test measures [1]
A. It measures the peripheral vision remaining on the client
B. Measures the Intra Ocular Pressure
C. Measures the Client’s Visual Acuity
D. Determines the Tone of the eye in response to the sudden increase in IOP.
* Tonometry measures the IOP. Normal range is 8 to 21 mmHg.
43. The Nurse notices that Mr. Batumbakal cannot anymore determine RED from BLUE. The nurse knew that which part of the eye is affected by this change? [3]
A. IRIS
B. PUPIL
c. RODS [RETINA]
D. CONES [RETINA]
* CONES Are responsible for COLOR VISION and DAY VISION, they are very sensitive to RED LIGHT that is why red lights are use to guide the elderly towards the bathroom when they wake up to urinate. Rods are responsible for night vision. They are sensitive to blue and green lights.
44. Nurse Jet knows that Aqueous Humor is produce where? [4]
A. In the sub arachnoid space of the meninges
B. In the Lateral ventricles
C. In the Choroids
D. In the Ciliary Body
* AH is produced in the CILIARY BODY. It is filtered by the trabecular meshwork into the canal of schlemm.
45. Nurse Jet knows that the normal IOP is [2]
A. 8-21 mmHg
B. 2-7 mmHg
c. 31-35 mmHg
D. 15-30 mmHg
46. Nurse Jet wants to measure Mr. Batumbakal’s CN II Function. What test would Nurse Jet implement to measure CN II’s Acuity? [1]
A. Slit lamp
B. Snellen’s Chart
C. Wood’s light
D. Gonioscopy
* CN II is the optic nerve. To assess its acuity, Snellen's chart is used. Slit lamp is the one you see in the usual Eye glasses shop where in, you need to look into its binocular-like holes and the optometrist is on the other side to magnify the structures of the eye to assess gross damage and structure. Woods light is a BLUE LIGHT used in dermatology. It is use to mark lesions usually caused skin infection. Gonioscopy is the angle measurement of the eye.
47. The Doctor orders pilocarpine. Nurse jet knows that the action of this drug is to [4]
A. Contract the Ciliary muscle
B. Relax the Ciliary muscle
C. Dilate the pupils
D. Decrease production of Aqueous Humor
* When the ciliary muscles contract, pupils constrict and the angle widens causing an increase AH outflow and decrease IOP. Relaxing the ciliary muscle will cause mydriasis or dilation, it is used as a pre op meds for cataract surgery and eye examination to better visualize the structures behind the iris. A and C are the same. Other drugs like betaxolol, Azetazolamide and epinephrine are the drugs used to decrease AH production.
48. The doctor orders timolol [timoptic]. Nurse jet knows that the action of this drug is [4]
A. Reduce production of CSF
B. Reduce production of Aqueous Humor
C. Constrict the pupil
D. Relaxes the Ciliary muscle
* All the eye drops the ends in OLOL decreases AH production. They are BETA BLOCKERS. Watch out for the S/S of congestive heart failure, bradycardia, hypotension and arrythmias.
49. When caring for Mr. Batumbakal, Jet teaches the client to avoid [1]
A. Watching large screen TVs
B. Bending at the waist
C. Reading books
D. Going out in the sun
* Bending at the waist increase IOP and should be avoided by patients with glaucoma. Treatment for glaucoma is usually for life. Patients are given laxatives to avoid stratining at the stool. They should avoid all activities that will lead to sudden IOP increase like bending at the waist. Clients should bend at the knees.
50. Mr. Batumbakal has undergone eye angiography using an Intravenous dye and fluoroscopy. What activity is contraindicated immediately after procedure? [4]
A. Reading newsprint
B. Lying down
C. Watching TV
D. Listening to the music
* The client had an eye angiography. Eye angiography requires the use MYDRIATICS pre-procedure. It is done by injecting an Intravenous dye and visualizes the flow of the dye throught the fluoroscopy along the vessels of the eye. This is to assess macular degeneration or neovascularizations [ proliferation of new vessels to compensate for continuous rupture and aneurysms of the existing vessels ] Mydratics usually takes 6 hours to a day to wear off. If client uses a mydratic, his pupil wil dilate making it UNABLE to focus on closer objects. Only A necessitates the constriction of the pupil to focus on a near object, which Mr.Batumbakals eye cannot perform at this time.
51. If Mr. Batumbakal is receiving pilocarpine, what drug should always be available in any case systemic toxicity occurs? [2]
A. Atropine Sulfate
B. Pindolol [Visken]
C. Naloxone Hydrochloride [Narcan]
D. Mesoridazine Besylate [Serentil]
* Atropine sulfate is use to reverse the effects of systemic toxicity of pilocarpine. Narcan is the antidote for respiratory depression caused by narcotics like morphine and demerol. Serentil is an antipsychotic.
SITUATION : Wide knowledge about the human ear, it’s parts and it’s functions will help a nurse assess and analyze changes in the adult client’s health.
52. Nurse Budek is doing a caloric testing to his patient, Aida, a 55 year old university professor who recently went into coma after being mauled by her disgruntled 3rd year nursing students whom she gave a failing mark. After instilling a warm water in the ear, Budek noticed a rotary nystagmus towards the irrigated ear. What does this means? [2]
A. Indicates a CN VIII Dysfunction
B. Abnormal
C. Normal
D. Inconclusive
* Rotary nystagmus towards the ear [ if warm ] or away from it [ if cool ] is a normal response. It indicates that the CN VIII Vestibular branch is still intact.
53. Ear drops are prescribed to an infant, The most appropriate method to administer the ear drops is [2]
A. Pull the pinna up and back and direct the solution towards the eardrum
B. Pull the pinna down and back and direct the solution onto the wall of the canal
C. Pull the pinna down and back and direct the solution towards the eardrum
D. Pull the pinna up and back and direct the solution onto the wall of the canal
* Instillation for children under age 3 is CHILD : DOWN AND BACK. Directing the solution towards the eardrum might perforate or damage the infants fragile tympanic membrane.
54. Nurse Budek is developing a plan of care for a patient with Menieres disease. What is the priority nursing intervention in the plan of care for this particular patient? [1]
A. Air, Breathing, Circulation
B. Love and Belongingness
C. Food, Diet and Nutrition
D. Safety
* Although A is priority according to maslow, it is not specific in clients with menieres disease. The client has an attack of incapacitating vertigo and client is high risk for injury due to falls. The client will perceive the environment moving due to disruption of the vestibular system of the ear's normal function.
55. After mastoidectomy, Nurse Budek should be aware that the cranial nerve that is usually damage after this procedure is [3]
A. CN I
B. CN II
C. CN VII
D. CN VI
* The facial nerve branches from the back of the ear and spread towards the mouth, cheeks, eyelids and almost all over the face. In mastoidectomy, Incision is made at the back of the ears to clear the mastoid air cells of the mastoid bone that is infected. Clients are at very high risk for CN VII injury because of this. Observation during the post op after mastoidectomy should revolve around assessing the client's CN VII integrity.
56. The physician orders the following for the client with Menieres disease. Which of the following should the nurse question? [1]
A. Dipenhydramine [Benadryl]
B. Atropine sulfate
C. Out of bed activities and ambulation
D. Diazepam [Valium]
* Clients with acute attack of Menieres are required to have bed rest with side rails up to prevent injury. During periods of incapacitating vertigo, patient's eyes will have rotary nystagmus because of the perception that the environment is moving. Patients are also observed to hold the side rails so hard because they thought they are going to fall. Benadryl is used in menieres due to its anti histamine effects. B and D are used to allay clients anxiety and apprehension.
57. Nurse Budek is giving dietary instruction to a client with Menieres disease. Which statement if made by the client indicates that the teaching has been successful? [1]
A. I will try to eat foods that are low in sodium and limit my fluid intake
B. I must drink atleast 3,000 ml of fluids per day
C. I will try to follow a 50% carbohydrate, 30% fat and 20% protein diet
D. I will not eat turnips, red meat and raddish
* Clients are advised to limite fluid and sodium intake as not to further cause accumulation of fluids in the endolymph. C is the diabetic diet. D are the foods not eaten when clients are about to have a guaiac test.
58. Peachy was rushed by his father, Steven into the hospital admission. Peachy is complaining of something buzzing into her ears. Nurse Budek assessed peachy and found out It was an insect. What should be the first thing that Nurse Budek should try to remove the insect out from peachy’s ear? [3]
A. Use a flashlight to coax the insect out of peachy’s ear
B. Instill an antibiotic ear drops
C. Irrigate the ear
D. Pick out the insect using a sterile clean forceps
* Lights can coax the insect out of the child's ear. This is the first measure employed in removing a live insect from the childs ear. Insects are not removed ALIVE, therfore, C and D are both wrong. Antibiotics has no effects since the child do not have any infection. If the insect did not come out after coaxing it with light, 2nd measure employs instillation of diluted alcohol or a mineral oil to kill the insect which is then removed using letter D.
59. Following an ear surgery, which statement if heard by Nurse Budek from the patient indicates a correct understanding of the post operative instructions? [2]
A. Activities are resumed within 5 days
B. I will make sure that I will clean my hair and face to prevent infection
C. I will use straw for drinking
D. I should avoid air travel for a while
* After ear surgery, Air travel is halted for a while. There is no need to restrict activities. The client is not allowed to shower for 7 days, Patient can clean himself using a sponge bath but avoids to shampoo or wet the face and hair. Straws are not used after ear surgery because sips increases pressure in the ear.
60. Nurse Budek will do a caloric testing to a client who sustained a blunt injury in the head. He instilled a cold water in the client’s right ear and he noticed that nystagmus occurred towards the left ear. What does this finding indicates? [2]
A. Indicating a Cranial Nerve VIII Dysfunction
B. The test should be repeated again because the result is vague
C. This is Grossly abnormal and should be reported to the neurosurgeon
D. This indicates an intact and working vestibular branch of CN VIII
* Refer to #52
61. A client with Cataract is about to undergo surgery. Nurse Budek is preparing plan of care. Which of the following nursing diagnosis is most appropriate to address the long term need of this type of patient? [1]
A. Anxiety R/T to the operation and its outcome
B. Sensory perceptual alteration R/T Lens extraction and replacement
C. Knowledge deficit R/T the pre operative and post operative self care
D. Body Image disturbance R/T the eye packing after surgery
* Patient do not have signs of anxiety, knowledge deficit or body image disturbance. The safest answer is B because before cataract surgery, client has a blurry vision that alters his sensory perception. After surgery client will be APHAKIC and again, will have an alteration in perception until the aphakic glass is available.
62. Nurse Budek is performing a WEBERS TEST. He placed the tuning fork in the patients forehead after tapping it onto his knee. The client states that the fork is louder in the LEFT EAR. Which of the following is a correct conclusion for nurse Budek to make? [4]
A. He might have a sensory hearing loss in the left ear
B. Conductive hearing loss is possible in the right ear
C. He might have a sensory hearing loss in the right hear, and/or a conductive hearing loss in the left ear.
D. He might have a conductive hearing loss in the right ear, and/or a sensory hearing loss in the left ear.
* Webers test assesses both air and bone conduction but is not decisive enough to judge which is which. When the tuning fork is tapped on the examiners knee, it is placed in the forehead or above the clients top lip. If the sound lateralizes towards the left ear, its either, the client has conductive hearing loss towards the left OR a sensory hearing loss in the right ear.
Why does conductive hearing produces a louder sound ?
Conductive hearing loss is a type of hearing loss where in, the ossicles hypertrophies, as in OTOSCLEROSIS. The stape is permanently attached to the oval window and it would not bulge causing a permanent LOUD conduction of sound using the bone because the stapes is already attached permanently into the inner ear. In a normal stape, It will not touch the oval window unless a sound is transmitted. [ refer to the ear anatomy and physiology ]
63. Aling myrna has Menieres disease. What typical dietary prescription would nurse Budek expect the doctor to prescribe? [2]
A. A low sodium , high fluid intake
B. A high calorie, high protein dietary intake
C. low fat, low sodium and high calorie intake
D. low sodium and restricted fluid intake
* Refer to # 57
SITUATION : [ From DEC 1991 NLE ] A 45 year old male construction worker was admitted to a tertiary hospital for incessant vomiting. Assessment disclosed: weak rapid pulse, acute weight loss of .5kg, furrows in his tongue, slow flattening of the skin was noted when the nurse released her pinch.
Temperature: 35.8 C , BUN Creatinine ratio : 10 : 1, He also complains for postural hypotension. There was no infection.
64. Which of the following is the appropriate nursing diagnosis? [1]
A. Fluid volume deficit R/T furrow tongue
B. Fluid volume deficit R/T uncontrolled vomiting
C. Dehydration R/T subnormal body temperature
D. Dehydration R/T incessant vomiting
65. Approximately how much fluid is lost in acute weight loss of .5kg? [1]
A. 50 ml
B. 750 ml
C. 500 ml
D. 75 ml
* 1L = 1kg
66. Postural Hypotension is [1]
A. A drop in systolic pressure less than 10 mmHg when patient changes position from lying to sitting.
B. A drop in systolic pressure greater than 10 mmHg when patient changes position from lying to sitting
C. A drop in diastolic pressure less than 10 mmHg when patient changes position from lying to sitting
D. A drop in diastolic pressure greater than 10 mmHg when patient changes position from lying to sitting
* Postural hypotension is exhibited by a drop of systolic BP when client changes position from lying to sitting or standing.
67. Which of the following measures will not help correct the patient’s condition [1]
A. Offer large amount of oral fluid intake to replace fluid lost
B. Give enteral or parenteral fluid
C. Frequent oral care
D. Give small volumes of fluid at frequent interval
* The patient will not tolerate large amount of oral fluid due to incessant vomiting.
68. After nursing intervention, you will expect the patient to have [1]
1. Maintain body temperature at 36.5 C
2. Exhibit return of BP and Pulse to normal
3. Manifest normal skin turgor of skin and tongue
4. Drinks fluids as prescribed
A. 1,3
B. 2,4
C. 1,3,4
D. 2,3,4
* Client need not maintain a temperature of 36.5 C. As long as the client will exhibit absence of fever or hypothermia, Nursing interventions are successfully carried out.
SITUATION: [ From JUN 2005 NLE ] A 65 year old woman was admitted for Parkinson’s Disease. The charge nurse is going to make an initial assessment.
69. Which of the following is a characteristic of a patient with advanced Parkinson’s disease? [1]
A. Disturbed vision
B. Forgetfulness
C. Mask like facial expression
D. Muscle atrophy
* Parkinson's disease does not affect the cognitive ability of a person. It is a disorder due to the depletion of the neurotransmitter dopamine which is needed for inhibitory control of muscular contractions. Client will exhibit mask like facial expression, Cog wheel rigidity, Bradykinesia, Shuffling gait etc. Muscle atrophy does not occur in parkinson's disease nor visual disturbances.
70. The onset of Parkinson’s disease is between 50-60 years old. This disorder is caused by [1]
A. Injurious chemical substances
B. Hereditary factors
C. Death of brain cells due to old age
D. Impairment of dopamine producing cells in the brain
* Dopamine producing cells in the basal ganglia mysteriously deteriorates due to unknown cause.
71. The patient was prescribed with levodopa. What is the action of this drug? [1]
A. Increase dopamine availability
B. Activates dopaminergic receptors in the basal ganglia
C. Decrease acetylcholine availability
D. Release dopamine and other catecholamine from neurological storage sites
* Levodopa is an altered form of dopamine. It is metabolized by the body and then converted into dopamine for brain's use thus increasing dopamine availability. Dopamine is not given directly because of its inability to cross the BBB.
72. You are discussing with the dietician what food to avoid with patients taking levodopa? [3]
A. Vitamin C rich food
B. Vitamin E rich food
C. Thiamine rich food
D. Vitamin B6 rich food
* Vitamin b6 or pyridoxine is avoided in patients taking levodopa because levodopa increases vitamin b6 availability leading to toxicity.
73. One day, the patient complained of difficulty in walking. Your response would be [2]
A. You will need a cane for support
B. Walk erect with eyes on horizon
C. I’ll get you a wheelchair
D. Don’t force yourself to walk
* Telling the client to walk erect neglects the clients complain of difficulty walking. Wheelchair is as much as possible not used to still enhance the client's motor function using a cane. Telling the client not to force himself walk is non therapeutic. The client wants to talk and we should help her walk using devices such as cane to provide support and prevent injuries.
SITUATION: [ From JUN 2005 NLE ] Mr. Dela Isla, a client with early Dementia exhibits thought process disturbances.
74. The nurse will assess a loss of ability in which of the following areas? [2]
A. Balance
B. Judgment
C. Speech
D. Endurance
* Perhaps this question from the JUN 2005 NLE is finding what should the nurse NOT assess because A,B and C are all affected by dementia except ENDURANCE, which is normally lost as a person ages. There will be alteration in balance because coordination and spatial ability gradually deteriorates. Judgement is also impaired as the client exhibits poor memory and concentration. Speech is severely altered. Client develops aphasia, agnosia and in at end, will lose all the ability to speak without any manifestation of motor problem.
75. Mr. Dela Isla said he cannot comprehend what the nurse was saying. He suffers from: [1]
A. Insomnia
B. Aphraxia
C. Agnosia
D. Aphasia
* This question was RECYCLED during the last 2006 NLE. Aphasia is the INABILITY to speak or understand. Aphraxia is the inability to carry out purposeful tasks. Agnosia is the inability to recognize familiar objects. Insomnia is the inability to fall asleep.
76. The nurse is aware that in communicating with an elderly client, the nurse will [1]
A. Lean and shout at the ear of the client
B. Open mouth wide while talking to the client
C. Use a low-pitched voice
D. Use a medium-pitched voice
* Talk as normally as possible. The client has dementia and is not deaf, although hearing might be impaired progressively as the client ages, the nurse should not alter his voice, shout or over enunciate the words. Client will preceive this things as belittling and direspectful.
77. As the nurse talks to the daughter of Mr. Dela Isla, which of the following statement of the daughter will require the nurse to give further teaching? [1]
A. I know the hallucinations are parts of the disease
B. I told her she is wrong and I explained to her what is right
C. I help her do some tasks he cannot do for himself
D. Ill turn off the TV when we go to another room
* Hallucinations and delusions are part of DEMENTIA and is termed as ORGANIC PSYCHOSES. The daughter needs further teaching when she try to bargain, explain, dissprove or advice a client with dementia. the client has an impaired judgement, concentration, thinking, reasoning and memory and has inability to learn that is why institutional care for clients with dementia is always required. The disease is progressive and is not preventable.
78. Which of the following is most important discharge teaching for Mr. Dela Isla [2]
A. Emergency Numbers
B. Drug Compliance
C. Relaxation technique
D. Dietary prescription
* Drug compliance is the most important teaching for Mr. Dela Isla to prevent the symptoms of psychoses and to control behavioral symptoms.
SITUATION : Knowledge of the drug PROPANTHELINE BROMIDE [Probanthine] Is necessary in treatment of various disorders.
79. What is the action of this drug? [4]
A. Increases glandular secretion for clients affected with cystic fibrosis
B. Dissolve blockage of the urinary tract due to obstruction of cystine stones
C. Reduces secretion of the glandular organ of the body
D. Stimulate peristalsis for treatment of constipation and obstruction
* Probanthine reduces glandular secretion of the different organs of the body. It is an anti-cholinergic / anti spasmodic drug and still, not approved by the FDA for treatment with various disorders. Probanthine exerts benifits for treatment of severe diaphoresis, Ulcers due to over secretion of HCl, Spasms, PANCREATITS [ Please take note ] and other conditions of over secretion.
80. What should the nurse caution the client when using this medication [4]
A. Avoid hazardous activities like driving, operating machineries etc.
B. Take the drug on empty stomach
C. Take with a full glass of water in treatment of Ulcerative colitis
D. I must take double dose if I missed the previous dose
* Like other anti cholinergics/ anti spasmodics, Probanthine causes dizziness, blurred vision and drowsiness. Patients are advised not to drive, operate heavy machineries etc. Probanthine should be taken with a full glass of water but is contraindicated with inflammatory bowel diseases like ulcerative colitis and chrons disease. Drug is taken with meals to prevent irritation of the gastric mucosa and client is advised not to take double dose in case the previous dose is missed.
81. Which of the following drugs are not compatible when taking Probanthine? [4]
A. Caffeine
B. NSAID
C. Acetaminophen
D. Alcohol
* Probanthine on its own already cause severe dizziness and drowsiness. Addition of alcohol will further depress the CNS and might lead to potentiation of the side effects of probanthine. A,B,C are not contraindicated when taking probanthine EXCEPT when the disease entity itself do not permit intake of such drugs like in Pancreatitis, NSAID is not use. Pain is controlled using probanthine and meperidine [ demerol ] in cases of acute pancreatitis.
82. What should the nurse tell clients when taking Probanthine? [4]
A. Avoid hot weathers to prevent heat strokes
B. Never swim on a chlorinated pool
C. Make sure you limit your fluid intake to 1L a day
D. Avoid cold weathers to prevent hypothermia
* Probanthine alters the ability of the body to secrete sweat. Telling the client to avoid hot weathers to prevent heat stroke is appropriate. Chlorinated pool is discouraged for patients undergoing skin radiation for skin cancer to prevent breakdown. Limiting fluid intake and avoiding cold weather are unecessary teachings.
83. Which of the following disease would Probanthine exert the much needed action for control or treatment of the disorder? [4]
A. Urinary retention
B. Peptic Ulcer Disease
C. Ulcerative Colitis
D. Glaucoma
* Probanthine is use in PUD to decrease gastric acid secretion. It is also used in Pancreatitis to rest the pancreas from over secretion of pancreatic enzyme and to prevent pain and spasm. Probanthine is contraindicated in clients with UC, Glaucoma. Since this is an anti spasmodic drug, Urinary retention will be a side effect.
SITUATION : [ From DEC 2000 NLE ] Mr. Franco, 70 years old, suddenly could not lift his spoons nor speak at breakfast. He was rushed to the hospital unconscious. His diagnosis was CVA.
84. Which of the following is the most important assessment during the acute stage of an unconscious patient like Mr. Franco? [1]
A. Level of awareness and response to pain
B. Papillary reflexes and response to sensory stimuli
C. Coherence and sense of hearing
D. Patency of airway and adequacy of respiration
* Airway is always a priority in an unconscious client. Refer to maslows hierarchy of needs for prioritization. Although this is not absolute, knowledge with pathophysiology will best lead you to the correct option.
85. Considering Mr. Franco’s conditions, which of the following is most important to include in preparing Franco’s bedside equipment? [1]
A. Hand bell and extra bed linen
B. Sandbag and trochanter rolls
C. Footboard and splint
D. Suction machine and gloves
* CVA patients has impaired swallowing ability and if not absent, depressed gag reflex. Client is at the highest risk for aspiration when eating or drinking that is why NGT is initiated early in the hospitalization. B prevent EXTERNAL ROTATION in hip or leg fracture. Footboards and splint prevents FOOTDROP seen in clients that has a severed peroneal nerve or prolonged immobilization usually due to fractures that eventually puts pressure on the peroneal nerve. A is not specific to clients with CVA.
86. What is the rationale for giving Mr. Franco frequent mouth care? [1]
A. He will be thirsty considering that he is doesn’t drink enough fluids
B. To remove dried blood when tongue is bitten during a seizure
C. The tactile stimulation during mouth care will hasten return to consciousness
D. Mouth breathing is used by comatose patient and it’ll cause oral mucosa dying and cracking.
* Client will be on NGT once comatose, A is removed first. Client with CVA MAY have seizures, but it is RARE enough that it must require a frequent mouth care, B is eliminated next. Knowing that tactile stimulation is done by touching the patient and not by peforming mouth care will lead you to letter D. Comatose patient uses the mouth to breathe predisposing himself to drying, cracking and infections.
87. One of the complications of prolonged bed rest is decubitus ulcer. Which of the following can best prevent its occurrence? [1]
A. Massage reddened areas with lotion or oils
B. Turn frequently every 2 hours
C. Use special water mattress
D. Keep skin clean and dry
* Frequent turning and positioning is the single most important nursing intervention to prevent ulcer formation. Skins are massaged but once the areas are reddened already [ CLASS I Ulcer ], It is not anymore massaged as not to prevent further breakdown. Lotions and Oils are not use in clients skin because it will further enhance skin breakdown. Water matress are used in BURN patients to limit the pressure on the skin by his own body weight. An alternating-inflatable air matress is much more compatible in periodic distribution of pressure in clients with prolong immobility. Keeping skin clean and dry is important but not as important as frequent turning and positioning.
88. If Mr. Franco’s Right side is weak, What should be the most accurate analysis by the nurse? [4]
A. Expressive aphasia is prominent on clients with right sided weakness
B. The affected lobe in the patient is the Right lobe
C. The client will have problems in judging distance and proprioception
D. Clients orientation to time and space will be much affected
* If the client's right side is weak, the affected lobe is the LEFT LOBE which is where the broca's area is located. Client will exhibit expressive aphasia, careful and slow movements and right sided weakness. Judging distance and proprioception is usually impaired in clients with RIGHT sided stroke. Telling that the clients orientation to time and space will be much affected is a blind shot analysis. This is seen on clients with severe and massive hemorrhagic stroke with recovery failure related to aneurysms producing long term and permanent coma. Mr. Franco right side is weak, not paralysed, meaning, some functions are still left intact.
SITUATION : [ From JUN 1988 NLE ] a 20 year old college student was rushed to the ER of PGH after he fainted during their ROTC drill. Complained of severe right iliac pain. Upon palpation of his abdomen, Ernie jerks even on slight pressure. Blood test was ordered. Diagnosis is acute appendicitis.
89. Which result of the lab test will be significant to the diagnosis? [1]
A. RBC : 4.5 TO 5 Million / cu. mm.
B. Hgb : 13 to 14 gm/dl.
C. Platelets : 250,000 to 500,000 cu.mm.
D. WBC : 12,000 to 13,000/cu.mm
* WBC increases with inflammation and infection.
90. Stat appendectomy was indicated. Pre op care would include all of the following except? [1]
A. Consent signed by the father
B. Enema STAT
C. Skin prep of the area including the pubis
D. Remove the jewelries
* Refer to ABDOMINAL ASSESSMENT : STORY TOWARDS MASTERY
91. Pre-anesthetic med of Demerol and atrophine sulfate were ordered to : [3]
A. Allay anxiety and apprehension
B. Reduce pain
C. Prevent vomiting
D. Relax abdominal muscle
* Pain is not reduced in appendicits. Clients are not given pain medication as to assess whether the appendix ruptured. A sudden relief of pain indicates the the appendix has ruptured and client will have an emergency appendectomy and prevent peritonitis. Demerol and Atropine are used to allay client's anxiety pre operatively.
92. Common anesthesia for appendectomy is [3]
A. Spinal
B. General
C. Caudal
D. Hypnosis
* Spinal anesthesia is the most common method used in appendectomy. Using this method, Only the area affected is anesthetized preventing systemic side effects of anesthetics like dizziness, hypotension and RR depression.
93. Post op care for appendectomy include the following except [1]
A. Early ambulation
B. Diet as tolerated after fully conscious
C. Nasogastric tube connect to suction
D. Deep breathing and leg exercise
* Client's peristalsis will return in 48 to 72 hours post-op therefore, Fluid and food are witheld until the bowel sounds returns. Remember that ALL PROCUDURES requiring GENERAL and SPINAL anesthesia above the nerves that supply the intestines will cause temporary paralysis of the bowel. Specially when the bowels are traumatized during the procedure, it may take longer for the intestinal peristalsis to resume.
94. Peritonitis may occur in ruptured appendix and may cause serious problems which are [2]
1. Hypovolemia, electrolyte imbalance
2. Elevated temperature, weakness and diaphoresis
3. Nausea and vomiting, rigidity of the abdominal wall
4. Pallor and eventually shock
A. 1 and 2
B. 2 and 3
C. 1,2,3
D. All of the above
* Peritonitis will cause all of the above symptoms. The peritoneum has a natural tendency to GUARD and become RIGID as to limit the infective exudate exchange inside the abdominal cavity. Hypovolemia and F&E imbalance are caused by severe nausea and vomiting in patients with peritonitis because of acute pain. As inflammation and infection spreads, fever and chills will become more apparent causing elevation in temperature, weakness and sweating. If peritonitis is left untreated, Client will become severely hypotensive leading to shock and death.
95. If after surgery the patient’s abdomen becomes distended and no bowel sounds appreciated, what would be the most suspected complication? [1]
A. Intussusception
B. Paralytic Ileus
C. Hemorrhage
D. Ruptured colon
* Paralytic Ileus is a mechanical bowel obstruction where in, the patients intestine fails to regain its motility. It is usually caused by surgery and anesthesia. Intusussusception, Appendicitis and Peritonitis also causes paralytic ileus.
96. NGT was connected to suction. In caring for the patient with NGT, the nurse must [2]
A. Irrigate the tube with saline as ordered
B. Use sterile technique in irrigating the tube
C. advance the tube every hour to avoid kinks
D. Offer some ice chips to wet lips
* NGT after appendectomy is used not to deliver nutrients but to decompress the GI tract because of the absence of peristalsis after appendectomy. The stomach and intestines are not sterile, Clean technique is sufficient during irrigation. NGT is placed and not anymore advanced as long as it already reach the stomach. Naso enteric tubes are the one that are advanced periodically until obstruction is reached in the intestine. The client still needs assessment and confirmation of the return of peristalsis before anything is given per orem. Irrigations are done to prevent obstruction in the tube.
97. When do you think the NGT tube be removed? [1]
A. When patient requests for it
B. Abdomen is soft and patient asks for water
C. Abdomen is soft and flatus has been expelled
D. B and C only
* When flatus is expelled, it means that peristalsis has returned and theres is no need for continuing the NGT.
Situation: Amanda is suffering from chronic arteriosclerosis Brain syndrome she fell while getting out of the bed one morning and was brought to the hospital, and she was diagnosed to have cerebrovascular thrombosis thus transferred to a nursing home.
98. What do you call a STROKE that manifests a bizarre behavior? [4]
A. Inorganic Stroke
B. Inorganic Psychoses
C. Organic Stroke
D. Organic Psychoses
* Organic psychoses is a broad and collective term used for psychoses and schizophrenia that has an organic cause. [ Due to Creutzfeldt jakob disease, huntington, hydrocephalus, increase ICP, dementia, stroke etc. ] Manifesting signs and symptoms like hallucination, delustions, illusion, ideas of reference etc. that is similar to schizophrenia and psychoses in absence of organic causes.
99. The main difference between chronic and organic brain syndrome is that the former [2]
A. Occurs suddenly and reversible
B. Is progressive and reversible
C. tends to be progressive and irreversible
D. Occurs suddenly and irreversible
* Chronic brain syndrome tends to be progressive and irreversible. Organic brain syndrome is acute and irreversible or reversible depending on the causative factor.
100. Which behavior results from organic psychoses? [4]
A. Memory deficit
B. Disorientation
C. Impaired Judgement
D. Inappropriate affect
* B, C and D are all behaviors that results from organic psychoses. The questions seems to ask EXCEPTION which is A. MEMORY DEFICIT. Organic psychoses is the same as the usual psychoses except that the causative factor of organic psychoses is evidently caused by a disease process of the brain or affecting the brain. Example are patients who suffer stroke suddenly experience hallucinations and delusions. Organic psychoses is simply a psychoses that has an IDENTIFIED CAUSE. Knowing this will lead you to understand that psychoses is manifested by B,C, and D but NOT MEMORY DEFICIT.
Psyche Nursing I
1. 60 year old post CVA patient is taking TPA for his disease, the nurse understands that this is an example of what level of prevention?
a. primary
b. secondary
c. tertiary
d. none of the above
2. A female client undergoes yearly mammography. This is a type of what level of prevention?
a. primary
b. secondary
c. tertiary
d. none of the above
3. A Diabetic patient was amputated following an unexpected necrosis on the right leg, he sustained and undergone BKA. He then underwent therapy on how to use his new prosthetic leg. this is a type of what level of prevention?
a. primary
b. secondary
c. tertiary
d. none of the above
4. As a care provider, The nurse should do first:
a. Provide direct nursing care.
b. Participate with the team in performing nursing intervention.
c. Therapeutic use of self.
d. Early recognition of the client’s needs.
5. As a manager, the nurse should:
a. Initiates nursing action with co workers.
b. Plans nursing care with the patient.
c. Speaks in behalf of the patient.
d. Works together with the team.
6. the nurse shows a patient advocate role when
a. defend the patients right
b. refer patient for other services she needs
c. work with significant others
d. intercedes in behalf of the patient.
7. which is the following is the most appropriate during the orientation phase ?
a. patients perception on the reason of her hospitalization
b. identification of more effective ways of coping
c. exploration of inadequate coping skills
d. establishment of regular meeting of schedules
8. preparing the client for the termination phase begins :
a. pre orientation
b. orientation
c. working
d. termination
9. a helping relationship is a process characterized by :
a. recovery promoting
b. mutual interaction
c. growth facilitating
d. health enhancing
10. During the nurse patient interaction, the nurse assess the ff: to determine the patients coping strategy :
a. how are you feeling right now?
b. do you have anyone to take you home?
c. what do you think will help you right now?
d. How does your problem affect your life?
11. As a counsellor, the nurse performs which of the ff: task?
a. encourage client to express feelings and concerns
b. helps client to learn a dance or song to enable her to participate in activities
c. help the client prepare in group activities
d. assist the client in setting limits on her behaviour
12. Freud stresses out that the EGO
a. Distinguishes between things in the mind and things in the reality.
b. Moral arm of the personality that strives for perfection than pleasure.
c. Reservoir of instincts and drives
d. Control the physical needs instincts.
13. A 16 year old child is hospitalized, according to Erik Erikson, what is an appropriate intervention?
a. tell the friends to visit the child
b. encourage patient to help child learn lessons missed
c. call the priest to intervene
d. tell the child’s girlfriend to visit the child.
14. NMS is characterized by :
a. hypertension, hyperthermia, flushed and dry skin.
b. Hypotension, hypothermia, flushed and dry skin.
c. Hypertension, hyperthermia, diaphoresis
d. Hypertension, hypothermia, diaphoresis
15. Which of the following drugs needs a WBC level checked regularly?
a. Lithane
b. Clozaril
c. Tofranil
d. Diazepam
Angelo, an 18 year old out of school youth was caught shoplifting in a department store. He has history of being quarrelsome and involving physical fight with his friends. He has been out of jail for the past two years
16. Initially, The nurse identifies which of the ff: Nursing diagnosis:
a. self centred disturbance
b. impaired social interaction
c. sensory perceptual alteration
d. altered thought process
17. which of the ff: is not a characteristic of PD?
a. disregard rights of others
b. loss of cognitive functioning
c. fails to conform to social norms
d. not capable of experiencing guild or remorse for their behaviour
18. the most effective treatment modality for persons if anti social PD is
a. hypnotherapy
b. gestalt therapy
c. behaviour therapy
d. crisis intervention
19. Which of the following is not an example of alteration of perception?
a. ideas of reference
b. flight of ideas
c. illusion
d. hallucination
20. The type of anxiety that leads to personality disorganization is :
a. Mild b. moderate c. severe d. panic
21. A client is admitted to the hospital. Twelve hours later the nurse observes hand tremors, hyperexicitability, tachycardia, diaphoresis and hypertension. The nurse suspects alcohol withdrawal. The nurse should ask the client:
a. at what time was your last drink taken?
b. Why didn’t you tell us you’re a drinker?
c. Do you drink beer or hard liquor?
d. How long have you been drinking?
22. client with a history of schizophrenia has been admitted for suicidal ideation. The client states "God is telling me to kill myself right now." The nurse's best response is:
a. I understand that god’s voice are real to you, But I don’t hear anything. I will stay with you.
b. The voices are part of your illness, it will stop if you take medication
c. The voices are all in your imagination, think of something else and itll go away
d. Don’t think of anything right now, just go and relax.
23. In assessing a client's suicide potential, which statement by the client would give the nurse the HIGHEST cause for concern?
a. my thoughts of hurting my self are scary to me
b. I’d like to go to sleep and not wake up
c. I’ve thought about taking pills and alcohol till I pass out
d. Id like to be free from all these worries
24. A client with paranoid schizophrenia has persecutory delusions and auditory hallucinations and is extremely agitated. He has been given a PRN dose of Thorazine IM. Which of the following would indicate to the nurse that the medication is having the desired effect?
a. Complains of dry mouth
b. State he feels restless in his body
c. Stops pacing and sits with the nurse
d. Exhibits increase activity and speech
25. A client who was wandering aimlessly around the streets acting inappropriately and appeared disheveled and unkempt was admitted to a psychiatric unit and is experiencing auditory and visual hallucinations. The nurse would develop a plan of care based on:
a. borderline personality disorder
b. anxiety disorder
c. schizophrenia
d. depression
26. A decision is made to not hospitalize a client with obsessive-compulsive disorder. Of the following abilities the client has demonstrated, the one that probably most influenced the decision not to hospitalize him is his ability to:
a. Hold a job.
b. Relate to his peers.
c. Perform activities of daily living.
d. Behave in an outwardly normal
27. A client is admitted to the inpatient psychiatric unit. He is unshaven, has body odor, and has spots on his shirt and pants. He moves slowly, gazes at the floor, and has a flat affect. The nurse's highest priority in assessing the client on admission would be to ask him:
a. How he sleeps at night.
b. If he is thinking about hurting himself.
c. About recent stresses.
d. How he feels about himself.
28. The nurse should know that the normal therapeutic level of lithium is :
a. .6 to 1.2 meq/L
b. 6 to 12 meq/L
c. .6 to .12 cc/ml
d. .6 to .12 cc3/L
29. The patient complaint of vomiting, diarrhea and restlessness after taking lithane. The nurse’s initial intervention is :
a. Recognize that this is a sign of toxicity and withhold the next medication.
b. Notify the physician.
c. Check V/S to validate patient’s concerns.
d. Recognize that this is a normal side effects of lithium and still continue the drug.
30. The client is taking TOFRANIL. The nurse should closely monitor the patient for :
a. Hypertension
b. Hypothermia
c. Increase Intra Ocular Pressure
d. Increase Intra Cranial Pressure
31. A client was hospitalized with major depression with suicidal ideation for 1 week. He is taking venlafaxine (Effexor), 75 mg three times a day, and is planning to return to work. The nurse asks the client if he is experiencing thoughts of self-harm. The client responds, "I hardly think about it anymore and wouldn't do anything to hurt myself." The nurse judges:
a. The client to be decompensating and in need of being readmitted to the hospital.
b. The client to need an adjustment or increase in his dose of antidepressant.
c. The depression to be improving and the suicidal ideation to be lessening.
d. The presence of suicidal ideation to warrant a telephone call to the client's physician
32. The client is taking sertraline (Zoloft), 50 mg q AM. The nurse includes which of the following in the teaching plan about Zoloft?
a. Zoloft causes erectile dysfunction in men.
b. Zoloft causes postural hypotension
c. Zoloft increases appetite and weight gain
d. It may take 3-4 weeks before client will start feeling better.
33. After 3 days of taking haloperidol, the client shows an inability to sit still, is restless and fidgety, and paces around the unit. Of the following extrapyramidal adverse reactions, the client is showing signs of:
a. Dystonia.
b. Akathisia.
c. Parkinsonism.
d. Tardive dyskinesia.
34. After 10 days of lithium therapy, the client's lithium level is 1.0 mEq/L. The nurse knows that this value indicates which of the following?
a. A laboratory error.
b. An anticipated therapeutic blood level of the drug.
c. An atypical client response to the drug.
d. A toxic level.
35. When caring for a client receiving haloperidol (Haldol), the nurse would assess for which of the following?
a. Hypertensive episodes.
b. Extrapyramidal symptoms.
c. Hypersalivation.
d. Oversedation.
36. A client is brought to the hospital’s emergency room by a friend, who states, "I guess he had some bad junk (heroin) today." In assessing the client, the nurse would likely find which of the following symptoms?
a. Increased heart rate, dilated pupils, and fever.
b. Tremulousness, impaired coordination, increased blood pressure, and ruddy complexion.
c. Decreased respirations, constricted pupils, and pallor.
d. Eye irritation, tinnitus, and irritation of nasal and oral mucosa.
37. The client has been taking the monoamine oxidase inhibitor (MAOI) phenelzine (Nardil), 10 mg bid. The physician orders a selective serotonin reuptake inhibitor (SSRI), paroxetine (Paxil), 20 mg given every morning. The nurse:
a. Gives the medication as ordered.
b. Questions the physician about the order.
c. Questions the dosage ordered.
d. Asks the physician to order benztropine (Cogentin) for the side effects.
38. Which of the following client statements about clozapine (Clozaril) indicates that the client needs additional teaching?
a. "I need to have my blood checked once every several months while I’m taking this drug."
b. "I need to sit on the side of the bed for a while when I wake up in the morning."
c. "The sleepiness I feel will decrease as my body adjusts to clozapine."
d. "I need to call my doctor whenever I notice that I have a fever or sore throat."
39. A client has been taking lithium carbonate (Lithane) for hyperactivity, as prescribed by his physician. While the client is taking this drug, the nurse should ensure that he has an adequate intake of:
a. Sodium.
b. Iron.
c. Iodine.
d. Calcium.
40. The client has been taking clomipramine (Anafranil) for his obsessive-compulsive disorder. He tells the nurse, "I'm not really better, and I've been taking the medication faithfully for the past 3 days just like it says on this prescription bottle." Which of the following actions would the nurse do first?
a. Tell the client to continue taking the medication as prescribed because it takes 5 to 10 weeks for a full therapeutic effect.
b. Tell the client to stop taking the medication and to call the physician.
c. Encourage the client to double the dose of his medication.
d. Ask the client if he has resumed smoking cigarettes.
41. The nurse judges correctly that a client is experiencing an adverse effect from amitriptyline hydrochloride (Elavil) when the client demonstrates:
a. An elevated blood glucose level.
b. Insomnia.
c. Hypertension.
d. Urinary retention.
42. Which of the following health status assessments must be completed before the client starts taking imipramine (Tofranil)?
a. Electrocardiogram (ECG).
b. Urine sample for protein.
c. Thyroid scan.
d. Creatinine clearance test.
43. A client comes to the outpatient mental health clinic 2 days after being discharged from the hospital. The client was given a 1-week supply of clozapine (Clozaril). The nurse reviews information about clozapine with the client. Which client statement indicates an accurate understanding of the nurse's teaching about this medication?
a."I need to call my doctor in 2 weeks for a checkup."
b."I need to keep my appointment here at the hospital this week for a blood test."
c. "I can drink alcohol with this medication."
d. "I can take over-the-counter sleeping medication if I have trouble sleeping."
44. The client is taking risperidone (Risperdal) to treat the positive and negative symptoms of schizophrenia. Which of the following negative symptoms will improve?.
a. Abnormal thought form.
b. Hallucinations and delusions.
c. Bizarre behaviour.
d. Asocial behaviour and anergia.
45. The nurse would teach the client taking tranylcypromine sulfate (Parnate) to avoid which food because of its high tyramine content?
a. Nuts.
b. Aged cheeses.
c. Grain cereals.
d. Reconstituted milk.
46. Which of the following clinical manifestations would alert the nurse to lithium toxicity?
a. Increasingly agitated behaviour.
b. Markedly increased food intake.
c. Sudden increase in blood pressure.
d.Anorexia with nausea and vomiting.
47. The client with depression has been hospitalized for 3 days on the psychiatric unit. This is the second hospitalization during the past year. The physician orders a different drug, tranylcypromine sulfate (Parnate), when the client does not respond positively to a tricyclic antidepressant. Which of the following reactions should the client be cautioned about if her diet includes foods containing tryaminetyramine?
a. Heart block.
b. Grand mal seizure.
c. Respiratory arrest.
d. Hypertensive crisis.
48. After the nurse has taught the client who is being discharged on lithium (Eskalith) about the drug, which of the following client statements would indicate that the teaching has been successful?
a. "I need to restrict eating any foods that contain salt."
b. "If I forget a dose, I can double the dose the next time I take it."
c. "I'll call my doctor right away for any vomiting, severe hand tremors, or muscle weakness."
d. "I should increase my fluid”
49. A nurse is caring for a client with Parkinson's disease who has been taking carbidopa/levodopa (Sinemet) for a year. Which of the following adverse reactions will the nurse monitor the client for?
a. dykinesia
b. glaucoma
c. hypotension
d. respiratory depression
50. A client is taking fluoxetine hydrochloride (Prozac) for treatment of depression. The client asks the nurse when the maximum therapeutic response occurs. The nurse's best response is that the maximum therapeutic response for fluoxetine hydrochloride may occur in the:
a. 10-14 days
b. First week
c. Third week
d. Fourth week
CLICK HERE FOR ANSWERS AND RATIONALE
Questions on Psychotic Disorders II
1. A psychotic client reports to the evening nurse that the day nurse put something suspicious in his water with his medication. The nurse replies, "You're worried about your medication?" The nurse's communication is:
A. an example of presenting reality.
B. reinforcing the client's delusions.
C. focusing on emotional content.
D. a nontherapeutic technique called mind reading.
2. A client is admitted to the inpatient unit of the mental health center with a diagnosis of paranoid schizophrenia. He's shouting that the government of France is trying to assassinate him. Which of the following responses is most appropriate?
A. "I think you're wrong. France is a friendly country and an ally of the United States. Their government wouldn't try to kill you."
B. "I find it hard to believe that a foreign government or anyone else is trying to hurt you. You must feel frightened by this."
C. "You're wrong. Nobody is trying to kill you."
D. "A foreign government is trying to kill you? Please tell me more about it."
3. Propranolol (Inderal) is used in the mental health setting to manage which of the following conditions?
A. Antipsychotic-induced akathisia and anxiety
B. The manic phase of bipolar illness as a mood stabilizer
C. Delusions for clients suffering from schizophrenia
D. Obsessive-compulsive disorder (OCD) to reduce ritualistic behavior
4. A client with borderline personality disorder becomes angry when he is told that today's psychotherapy session with the nurse will be delayed 30 minutes because of an emergency. When the session finally begins, the client expresses anger. Which response by the nurse would be most helpful in dealing with the client's anger?
A. "If it had been your emergency, I would have made the other client wait."
B. "I know it's frustrating to wait. I'm sorry this happened."
C. "You had to wait. Can we talk about how this is making you feel right now?"
D. "I really care about you and I'll never let this happen again."
5. How soon after chlorpromazine (Thorazine) administration should the nurse expect to see a client's delusional thoughts and hallucinations eliminated
A. Several minutes
B. Several hours
C. Several days
D. Several weeks
6. A client receiving haloperidol (Haldol) complains of a stiff jaw and difficulty swallowing. The nurse's first action is to:
A. reassure the client and administer as needed lorazepam (Ativan) I.M.
B. administer as needed dose of benztropine (Cogentin) I.M. as ordered.
C. administer as needed dose of benztropine (Cogentin) by mouth as ordered.
D. administer as needed dose of haloperidol (Haldol) by mouth.
7. A client with a diagnosis of paranoid schizophrenia comments to the nurse, "How do I know what is really in those pills?" Which of the following is the best response?
A. Say, "You know it's your medicine."
B. Allow him to open the individual wrappers of the medication.
C. Say, "Don't worry about what is in the pills. It's what is ordered."
D. Ignore the comment because it's probably a joke.
8. The nurse is caring for a client with schizophrenia who experiences auditory hallucinations. The client appears to be listening to someone who isn't visible. He gestures, shouts angrily, and stops shouting in mid-sentence. Which nursing intervention is the most appropriate?
A. Approach the client and touch him to get his attention.
B. Encourage the client to go to his room where he'll experience fewer distractions.
C. Acknowledge that the client is hearing voices but make it clear that the nurse doesn't hear these voices.
D. Ask the client to describe what the voices are saying.
9. Yesterday, a client with schizophrenia began treatment with haloperidol (Haldol). Today, the nurse notices that the client is holding his head to one side and complaining of neck and jaw spasms. What should the nurse do?
A. Assume that the client is posturing.
B. Tell the client to lie down and relax.
C. Evaluate the client for adverse reactions to haloperidol.
D. Put the client on the list for the physician to see tomorrow
10. A client with paranoid schizophrenia has been experiencing auditory hallucinations for many years. One approach that has proven to be effective for hallucinating clients is to:
A. take an as-needed dose of psychotropic medication whenever they hear voices.
B. practice saying "Go away" or "Stop" when they hear voices.
C. sing loudly to drown out the voices and provide a distraction.
D. go to their room until the voices go away.
11. A client with catatonic schizophrenia is mute, can't perform activities of daily living, and stares out the window for hours. What is the nurse's first priority?
A. Assist the client with feeding.
B. Assist the client with showering.
C. Reassure the client about safety.
D. Encourage socialization with peers.
12. A client tells the nurse that the television newscaster is sending a secret message to her. The nurse suspects the client is experiencing:
A. a delusion.
B. flight of ideas.
C. ideas of reference.
D. a hallucination.
13. The nurse knows that the physician has ordered the liquid form of the drug chlorpromazine (Thorazine) rather than the tablet form because the liquid:
A. has a more predictable onset of action.
B. produces fewer anticholinergic effects.
C. produces fewer drug interactions.
D. has a longer duration of action.
14. A client who has been hospitalized with disorganized type schizophrenia for 8 years can't complete activities of daily living (ADLs) without staff direction and assistance. The nurse formulates a nursing diagnosis of Self-care deficient: Dressing/grooming related to inability to function without assistance. What is an appropriate goal for this client?
A. "Client will be able to complete ADLs independently within 1 month."
B. "Client will be able to complete ADLs with only verbal encouragement within 1 month."
C. "Client will be able to complete ADLs with assistance in organizing grooming items and clothing within 1 month."
D. "Client will be able to complete ADLs with complete assistance within 1 month."
15. The nurse is planning care for a client admitted to the psychiatric unit with a diagnosis of paranoid schizophrenia. Which nursing diagnosis should receive the highest priority?
A. Risk for violence toward self or others
B. Imbalanced nutrition: Less than body requirements
C. Ineffective family coping
D. Impaired verbal communication
16. The nurse is preparing for the discharge of a client who has been hospitalized for paranoid schizophrenia. The client's husband expresses concern over whether his wife will continue to take her daily prescribed medication. The nurse should inform him that:
A. his concern is valid but his wife is an adult and has the right to make her own decisions.
B. he can easily mix the medication in his wife's food if she stops taking it.
C. his wife can be given a long-acting medication that is administered every 1 to 4 weeks.
D. his wife knows she must take her medication as prescribed to avoid future hospitalizations.
17. Benztropine (Cogentin) is used to treat the extrapyramidal effects induced by antipsychotics. This drug exerts its effect by:
A. decreasing the anxiety causing muscle rigidity.
B. blocking the cholinergic activity in the central nervous system (CNS).
C. increasing the level of acetylcholine in the CNS.
D. increasing norepinephrine in the CNS.
18. A client is admitted to the inpatient unit of the mental health center with a diagnosis of paranoid schizophrenia. He's shouting that the government of France is trying to assassinate him. Which of the following responses is most appropriate?
A. "I think you're wrong. France is a friendly country and an ally of the United States. Their government wouldn't try to kill you."
B. "I find it hard to believe that a foreign government or anyone else is trying to hurt you. You must feel frightened by this."
C. "You're wrong. Nobody is trying to kill you."
D. "A foreign government is trying to kill you? Please tell me more about it."
19. A dopamine receptor agonist such as bromocriptine (Parlodel) relieves muscle rigidity caused by antipsychotic medication by:
A. blocking dopamine receptors in the central nervous system (CNS).
B. blocking acetylcholine in the CNS.
C. activating norepinephrine in the CNS.
D. activating dopamine receptors in the CNS.
20. Most antipsychotic medications exert which of following effects on the central nervous system (CNS)?
A. Stimulate the CNS by blocking postsynaptic dopamine, norepinephrine, and serotonin receptors.
B. Sedate the CNS by stimulating serotonin at the synaptic cleft.
C. Depress the CNS by blocking the postsynaptic transmission of dopamine, serotonin, and norepinephrine.
D. Depress the CNS by stimulating the release of acetylcholine.
21. A client is admitted to the psychiatric unit of a local hospital with chronic undifferentiated schizophrenia. During the next several days, the client is seen laughing, yelling, and talking to herself. This behavior is characteristic of:
A. delusion.
B. looseness of association.
C. illusion.
D. hallucination.
22. Which of the following medications would the nurse expect the physician to order to reverse a dystonic reaction?
A. prochlorperazine (Compazine)
B. diphenhydramine (Benadryl)
C. haloperidol (Haldol)
D. midazolam (Versed)
23. A schizophrenic client states, "I hear the voice of King Tut." Which response by the nurse would be most therapeutic?
A. "I don't hear the voice, but I know you hear what sounds like a voice."
B. "You shouldn't focus on that voice."
C. "Don't worry about the voice as long as it doesn't belong to anyone real."
D. "King Tut has been dead for years."
24. A psychotic client reports to the evening nurse that the day nurse put something suspicious in his water with his medication. The nurse replies, "You're worried about your medication?" The nurse's communication is:
A. an example of presenting reality.
B. reinforcing the client's delusions.
C. focusing on emotional content.
D. a nontherapeutic technique called mind reading.
25. The nurse is caring for a client with schizophrenia who experiences auditory hallucinations. The client appears to be listening to someone who isn't visible. He gestures, shouts angrily, and stops shouting in mid-sentence. Which nursing intervention is the most appropriate?
A. Approach the client and touch him to get his attention.
B. Encourage the client to go to his room where he'll experience fewer distractions.
C. Acknowledge that the client is hearing voices but make it clear that the nurse doesn't hear these voices.
D. Ask the client to describe what the voices are saying
26. A client has been receiving chlorpromazine (Thorazine), an antipsychotic, to treat his psychosis. Which findings should alert the nurse that the client is experiencing pseudoparkinsonism?
A. Restlessness, difficulty sitting still, and pacing
B. Involuntary rolling of the eyes
C. Tremors, shuffling gait, and masklike face
D. Extremity and neck spasms, facial grimacing, and jerky movements
27. For several years, a client with chronic schizophrenia has received 10 mg of fluphenazine hydrochloride (Prolixin) by mouth four times per day. Now the client has a temperature of 102° F (38.9° C), a heart rate of 120 beats/minute, a respiratory rate of 20 breaths/minute, and a blood pressure of 210/140 mm Hg. Because the client also is confused and incontinent, the nurse suspects malignant neuroleptic syndrome. What steps should the nurse take?
A. Give the next dose of fluphenazine, call the physician, and monitor vital signs.
B. Withhold the next dose of fluphenazine, call the physician, and monitor vital signs.
C. Give the next dose of fluphenazine and restrict the client to the room to decrease stimulation.
D. Withhold the next dose of fluphenazine, administer an antipyretic agent, and increase the client's fluid intake.
28. A schizophrenic client with delusions tells the nurse, "There is a man wearing a red coat who's out to get me." The client exhibits increasing anxiety when focusing on the delusions. Which of the following would be the best response?
A. "This subject seems to be troubling you. Let's walk to the activity room."
B. "Describe the man who's out to get you. What does he look like?"
C. "There is no reason to be afraid of that man. This hospital is very secure."
D. "There is no need to be concerned with a man who isn't even real."
29. Important teaching for women in their childbearing years who are receiving antipsychotic medications includes which of the following?
A. Occurrence of increased libido due to medication adverse effects
B. Increased incidence of dysmenorrhea while taking the drug
C. Continuing previous use of contraception during periods of amenorrhea
D. Instruction that amenorrhea is irreversible
30. A client is admitted to a psychiatric facility with a diagnosis of chronic schizophrenia. The history indicates that the client has been taking neuroleptic medication for many years. Assessment reveals unusual movements of the tongue, neck, and arms. Which condition should the nurse suspect?
A. Tardive dyskinesia
B. Dystonia
C. Neuroleptic malignant syndrome
D. Akathisia
31. What medication would probably be ordered for the acutely aggressive schizophrenic client?
A. chlorpromazine (Thorazine)
B. haloperidol (Haldol)
C. lithium carbonate (Lithonate)
D. amitriptyline (Elavil)
32. A client is admitted with a diagnosis of schizotypal personality disorder. Which signs would this client exhibit during social situations?
A. Aggressive behavior
B. Paranoid thoughts
C. Emotional affect
D. Independence needs
33. During the initial interview, a client with schizophrenia suddenly turns to the empty chair beside him and whispers, "Now just leave. I told you to stay home. There isn't enough work here for both of us!" What is the nurse's best initial response?
A. "When people are under stress, they may see things or hear things that others don't. Is that what just happened?"
B. "I'm having a difficult time hearing you. Please look at me when you talk."
C. "There is no one else in the room. What are you doing?"
D. "Who are you talking to? Are you hallucinating?"
34. The definition of nihilistic delusions is:
A. a false belief about the functioning of the body.
B. belief that the body is deformed or defective in a specific way.
C. false ideas about the self, others, or the world.
D. the inability to carry out motor activities.
35. A client who's taking antipsychotic medication develops a very high temperature, severe muscle rigidity, tachycardia, and rapid deterioration in mental status. The nurse suspects what complication of antipsychotic therapy?
A. Agranulocytosis
B. Extrapyramidal effects
C. Anticholinergic effects
D. Neuroleptic malignant syndrome (NMS)
36. The nurse formulates a nursing diagnosis of Impaired social interaction related to disorganized thinking for a client with schizotypal personality disorder. Based on this nursing diagnosis, which nursing intervention takes highest priority?
A. Helping the client to participate in social interactions
B. Establishing a one-on-one relationship with the client
C. Exploring the effects of the client's behavior on social interactions
D. Developing a schedule for the client's participation in social interactions
37. A client with schizophrenia hears a voice telling him he is evil and must die. The nurse understands that the client is experiencing:
A. a delusion.
B. flight of ideas.
C. ideas of reference.
D. a hallucination.
38. A client with delusional thinking shows a lack of interest in eating at meal times. She states that she is unworthy of eating and that her children will die if she eats. Which nursing action would be most appropriate for this client?
A. Telling the client that she may become sick and die unless she eats
B. Paying special attention to the client's rituals and emotions associated with meals
C. Restricting the client's access to food except at specified meal and snack times
D. Encouraging the client to express her feelings at meal times
39. Which of the following groups of characteristics would the nurse expect to see in the client with schizophrenia?
A. Loose associations, grandiose delusions, and auditory hallucinations
B. Periods of hyperactivity and irritability alternating with depression
C. Delusions of jealousy and persecution, paranoia, and mistrust
D. Sadness, apathy, feelings of worthlessness, anorexia, and weight loss
40. The nurse must administer a medication to reverse or prevent Parkinson-type symptoms in a client receiving an antipsychotic. The medication the client will likely receive is:
A. benztropine (Cogentin).
B. diphenhydramine (Benadryl).
C. propranolol (Inderal).
D. haloperidol (Haldol).
41. A client is receiving haloperidol (Haldol) to reduce psychotic symptoms. As he watches television with other clients, the nurse notes that he has trouble sitting still. He seems restless, constantly moving his hands and feet and changing position. When the nurse asks what is wrong, he says he feels jittery. How should the nurse manage this situation?
A. Ask the client to sit still or leave the room because he is distracting the other clients.
B. Ask the client if he is nervous or anxious about something.
C. Give an as needed dose of a prescribed anticholinergic agent to control akathisia.
D. Administer an as needed dose of haloperidol to decrease agitation.
42. A man is brought to the hospital by his wife, who states that for the past week her husband has refused all meals and accused her of trying to poison him. During the initial interview, the client's speech, only partly comprehensible, reveals that his thoughts are controlled by delusions that he is possessed by the devil. The physician diagnoses paranoid schizophrenia. Schizophrenia is best described as a disorder characterized by:
A. disturbed relationships related to an inability to communicate and think clearly.
B. severe mood swings and periods of low to high activity.
C. multiple personalities, one of which is more destructive than the others.
D. auditory and tactile hallucinations.
43. A client has a history of chronic undifferentiated schizophrenia. Because she has a history of noncompliance with antipsychotic therapy, she'll receive fluphenazine decanoate (Prolixin Decanoate) injections every 4 weeks. Before discharge, what should the nurse include in her teaching plan?
A. Asking the physician for droperidol (Inapsine) to control any extrapyramidal symptoms that occur
B. Sitting up for a few minutes before standing to minimize orthostatic hypotension
C. Notifying the physician if her thoughts don't normalize within 1 week
D. Expecting symptoms of tardive dyskinesia to occur and to be transient
44. A client with chronic schizophrenia who takes neuroleptic medication is admitted to the psychiatric unit. Nursing assessment reveals rigidity, fever, hypertension, and diaphoresis. These findings suggest which life-threatening reaction:
A. tardive dyskinesia.
B. dystonia.
C. neuroleptic malignant syndrome.
D. akathisia.
45. While looking out the window, a client with schizophrenia remarks, "That school across the street has creatures in it that are waiting for me." Which of the following terms best describes what the creatures represent?
A. Anxiety attack
B. Projection
C. Hallucination
D. Delusion
46. A client with schizophrenia tells the nurse, "My intestines are rotted from the worms chewing on them." This statement indicates a:
A. delusion of persecution.
B. delusion of grandeur.
C. somatic delusion.
D. jealous delusion.
47. During the assessment stage, a client with schizophrenia leaves his arm in the air after the nurse has taken his blood pressure. His action shows evidence of:
A. somatic delusions.
B. waxy flexibility.
C. neologisms.
D. nihilistic delusions.
48. A client with paranoid type schizophrenia becomes angry and tells the nurse to leave him alone. The nurse should
A. tell him that she'll leave for now but will return soon.
B. ask him if it's okay if she sits quietly with him.
C. ask him why he wants to be left alone.
D. tell him that she won't let anything happen to him
49. Nursing care for a client with schizophrenia must be based on valid psychiatric and nursing theories. The nurse's interpersonal communication with the client and specific nursing interventions must be:
A. clearly identified with boundaries and specifically defined roles.
B. warm and nonthreatening.
C. centered on clearly defined limits and expression of empathy.
D. flexible enough for the nurse to adjust the plan of care as the situation warrants.
50. When discharging a client after treatment for a dystonic reaction, the emergency department nurse must ensure that the client understands which of the following?
A. Results of treatment are rapid and dramatic but may not last.
B. Although uncomfortable, this reaction isn't serious.
C. The client shouldn't buy drugs on the street.
D. The client must take benztropine (Cogentin) as prescribed to prevent a return of symptoms.
51. The nurse is caring for a client with schizophrenia. Which of the following outcomes is the least desirable?
A. The client spends more time by himself.
B. The client doesn't engage in delusional thinking.
C. The client doesn't harm himself or others.
D. The client demonstrates the ability to meet his own self-care needs.
52. The nurse formulates a nursing diagnosis of Impaired verbal communication for a client with schizotypal personality disorder. Based on this nursing diagnosis, which nursing intervention is most appropriate?
A. Helping the client to participate in social interactions
B. Establishing a one-on-one relationship with the client
C. Establishing alternative forms of communication
D. Allowing the client to decide when he wants to participate in verbal communication with the nurse
53. Since admission 4 days ago, a client has refused to take a shower, stating, "There are poison crystals hidden in the showerhead. They'll kill me if I take a shower." Which nursing action is most appropriate?
A. Dismantling the showerhead and showing the client that there is nothing in it
B. Explaining that other clients are complaining about the client's body odor
C. Asking a security officer to assist in giving the client a shower
D. Accepting these fears and allowing the client to take a sponge bath
54. Drug therapy with thioridazine (Mellaril) shouldn't exceed a daily dose of 800 mg to prevent which adverse reaction?
A. Hypertension
B. Respiratory arrest
C. Tourette syndrome
D. Retinal pigmentation
A. "I get upset once in a while, too."
B. "I know just how you feel. I'd feel the same way in your situation."
C. "I worry, too, when I think people are talking about me."
D. "At times, it's normal not to trust anyone."
56. How soon after chlorpromazine (Thorazine) administration should the nurse expect to see a client's delusional thoughts and hallucinations eliminated?
A. Several minutes
B. Several hours
C. Several days
D. Several weeks
57. A client is about to be discharged with a prescription for the antipsychotic agent haloperidol (Haldol), 10 mg by mouth twice per day. During a discharge teaching session, the nurse should provide which instruction to the client?
A. Take the medication 1 hour before a meal.
B. Decrease the dosage if signs of illness decrease.
C. Apply a sunscreen before being exposed to the sun.
D. Increase the dosage up to 50 mg twice per day if signs of illness don't decrease.
58. A client with paranoid schizophrenia repeatedly uses profanity during an activity therapy session. Which response by the nurse would be most appropriate?
A. "Your behavior won't be tolerated. Go to your room immediately."
B. "You're just doing this to get back at me for making you come to therapy."
C. "Your cursing is interrupting the activity. Take time out in your room for 10 minutes."
D. "I'm disappointed in you. You can't control yourself even for a few minutes."
59. Which of the following is one of the advantages of the newer antipsychotic medication risperidone (Risperdal)?
A. The absence of anticholinergic effects
B. A lower incidence of extrapyramidal effects
C. Photosensitivity and sedation
D. No incidence of neuroleptic malignant syndrome
60. The etiology of schizophrenia is best described by:
A. genetics due to a faulty dopamine receptor.
B. environmental factors and poor parenting.
C. structural and neurobiological factors.
D. a combination of biological, psychological, and environmental factors.
61. A client with schizophrenia who receives fluphenazine (Prolixin) develops pseudoparkinsonism and akinesia. What drug would the nurse administer to minimize extrapyramidal symptoms?
A. benztropine (Cogentin)
B. dantrolene (Dantrium)
C. clonazepam (Klonopin)
D. diazepam (Valium)
62. A client with a diagnosis of paranoid schizophrenia comments to the nurse, "How do I know what is really in those pills?" Which of the following is the best response?
A. Say, "You know it's your medicine."
B. Allow him to open the individual wrappers of the medication.
C. Say, "Don't worry about what is in the pills. It's what is ordered."
D. Ignore the comment because it's probably a joke.
63. A client tells the nurse that people from Mars are going to invade the earth. Which response by the nurse would be most therapeutic?
A. "That must be frightening to you. Can you tell me how you feel about it?"
B. "There are no people living on Mars."
C. "What do you mean when you say they're going to invade the earth?"
D. "I know you believe the earth is going to be invaded, but I don't believe that."
64. A client with schizophrenia tells the nurse he hears the voices of his dead parents. To help the client ignore the voices, the nurse should recommend that he:
A. sit in a quiet, dark room and concentrate on the voices.
B. listen to a personal stereo through headphones and sing along with the music.
C. call a friend and discuss the voices and his feelings about them.
D. engage in strenuous exercise.
65. A client with schizophrenia is receiving antipsychotic medication. Which nursing diagnosis may be appropriate for this client?
A. Ineffective protection related to blood dyscrasias
B. Urinary frequency related to adverse effects of antipsychotic medication
C. Risk for injury related to a severely decreased level of consciousness
D. Risk for injury related to electrolyte disturbances
66. A client with persistent, severe schizophrenia has been treated with phenothiazines for the past 17 years. Now the client's speech is garbled as a result of drug-induced rhythmic tongue protrusion. What is another name for this extrapyramidal symptom?
A. Dystonia
B. Akathisia
C. Pseudoparkinsonism
D. Tardive dyskinesia
67. The nurse is assigned to a client with catatonic schizophrenia. Which intervention should the nurse include in the client's plan of care?
A. Meeting all of the client's physical needs
B. Giving the client an opportunity to express concerns
C. Administering lithium carbonate (Lithonate) as prescribed
D. Providing a quiet environment where the client can be alone
68. A client with a history of medication noncompliance is receiving outpatient treatment for chronic undifferentiated schizophrenia. The physician is most likely to prescribe which medication for this client?
A. chlorpromazine (Thorazine)
B. imipramine (Tofranil)
C. lithium carbonate (Lithane)
D. fluphenazine decanoate (Prolixin Decanoate)
69. Propranolol (Inderal) is used in the mental health setting to manage which of the following conditions?
A. Antipsychotic-induced akathisia and anxiety
B. The manic phase of bipolar illness as a mood stabilizer
C. Delusions for clients suffering from schizophrenia
D. Obsessive-compulsive disorder (OCD) to reduce ritualistic behavior
70. Every day for the past 2 weeks, a client with schizophrenia stands up during group therapy and screams, "Get out of here right now! The elevator bombs are going to explode in 3 minutes!" The next time this happens, how should the nurse respond?
A. "Why do you think there is a bomb in the elevator?"
B. "That is the same thing you said in yesterday's session."
C. "I know you think there are bombs in the elevator, but there aren't."
D. "If you have something to say, you must do it according to our group rules."
71. A 26-year-old client is admitted to the psychiatric unit with acute onset of schizophrenia. His physician prescribes the phenothiazine chlorpromazine (Thorazine), 100 mg by mouth four times per day. Before administering the drug, the nurse reviews the client's medication history. Concomitant use of which drug is likely to increase the risk of extrapyramidal effects?
A. guanethidine (Ismelin)
B. droperidol (Inapsine)
C. lithium carbonate (Lithonate)
D. alcohol
72. A client, age 36, with paranoid schizophrenia believes the room is bugged by the Central Intelligence Agency and that his roommate is a foreign spy. The client has never had a romantic relationship, has no contact with family members, and hasn't been employed in the last 14 years. Based on Erikson's theories, the nurse should recognize that this client is in which stage of psychosocial development?
A. Autonomy versus shame and doubt
B. Generativity versus stagnation
C. Integrity versus despair
D. Trust versus mistrust
73. During a group therapy session in the psychiatric unit, a client constantly interrupts with impulsive behavior and exaggerated stories that cast her as a hero or princess. She also manipulates the group with attention-seeking behaviors, such as sexual comments and angry outbursts. The nurse realizes that these behaviors are typical of:
A. paranoid personality disorder.
B. avoidant personality disorder.
C. histrionic personality disorder.
D. borderline personality disorder.
74. The nurse is teaching a psychiatric client about her prescribed drugs, chlorpromazine and benztropine. Why is benztropine administered?
A. To reduce psychotic symptoms
B. To reduce extrapyramidal symptoms
C. To control nausea and vomiting
D. To relieve anxiety
75. A client is admitted to the psychiatric unit with a tentative diagnosis of psychosis. Her physician prescribes the phenothiazine thioridazine (Mellaril) 50 mg by mouth three times per day. Phenothiazines differ from central nervous system (CNS) depressants in their sedative effects by producing:
A. deeper sleep than CNS depressants.
B. greater sedation than CNS depressants.
C. a calming effect from which the client is easily aroused.
D. more prolonged sedative effects, making the client more difficult to arouse.
A. Schizophrenia
B. Paranoid personality
C. Bipolar illness
D. Obsessive-compulsive disorder (OCD)
77. A client with paranoid schizophrenia is admitted to the psychiatric unit of a hospital. Nursing assessment should include careful observation of the client's:
A. thinking, perceiving, and decision-making skills.
B. verbal and nonverbal communication processes.
C. affect and behavior.
D. psychomotor activity.
78. Which information is most important for the nurse to include in a teaching plan for a schizophrenic client taking clozapine (Clozaril)?
A. Monthly blood tests will be necessary.
B. Report a sore throat or fever to the physician immediately.
C. Blood pressure must be monitored for hypertension.
D. Stop the medication when symptoms subside.
79. Important teaching for clients receiving antipsychotic medication such as haloperidol (Haldol) includes which of the following instructions?
A. Use sunscreen because of photosensitivity.
B. Take the antipsychotic medication with food.
C. Have routine blood tests to determine levels of the medication.
D. Abstain from eating aged cheese.
80. Positive symptoms of schizophrenia include which of the following?
A. Hallucinations, delusions, and disorganized thinking
B. Somatic delusions, echolalia, and a flat affect
C. Waxy flexibility, alogia, and apathy
D. Flat affect, avolition, and anhedonia
81. A client with chronic schizophrenia receives 20 mg of fluphenazine decanoate (Prolixin Decanoate) by I.M. injection. Three days later, the client has muscle contractions that contort the neck. This client is exhibiting which extrapyramidal reaction?
A. Dystonia
B. Akinesia
C. Akathisia
D. Tardive dyskinesia
82. Hormonal effects of the antipsychotic medications include which of the following?
A. Retrograde ejaculation and gynecomastia
B. Dysmenorrhea and increased vaginal bleeding
C. Polydipsia and dysmenorrhea
D. Akinesia and dysphasia
83. A client is unable to get out of bed and get dressed unless the nurse prompts every step. This is an example of which behavior?
A. Word salad
B. Tangential
C. Perseveration
D. Avolition
84. An agitated and incoherent client, age 29, comes to the emergency department with complaints of visual and auditory hallucinations. The history reveals that the client was hospitalized for paranoid schizophrenia from ages 20 to 21. The physician prescribes haloperidol (Haldol), 5 mg I.M. The nurse understands that this drug is used in this client to treat:
A. dyskinesia.
B. dementia.
C. psychosis.
D. tardive dyskinesia.
85. Yesterday, a client with schizophrenia began treatment with haloperidol (Haldol). Today, the nurse notices that the client is holding his head to one side and complaining of neck and jaw spasms. What should the nurse do?
A. Assume that the client is posturing.
B. Tell the client to lie down and relax.
C. Evaluate the client for adverse reactions to haloperidol.
D. Put the client on the list for the physician to see tomorrow.
86. A client receiving fluphenazine decanoate (Prolixin Decanoate) therapy develops pseudoparkinsonism. The physician is likely to prescribe which drug to control this extrapyramidal effect?
A. phenytoin (Dilantin)
B. amantadine (Symmetrel)
C. benztropine (Cogentin)
D. diphenhydramine (Benadryl)
87. Important teaching for a client receiving risperidone (Risperdal) would include advising the client to:
A. double the dose if missed to maintain a therapeutic level.
B. be sure to take the drug with a meal because it's very irritating to the stomach.
C. discontinue the drug if the client reports weight gain.
D. notify the physician if the client notices an increase in bruising.
88. A client is admitted to the psychiatric hospital with a diagnosis of catatonic schizophrenia. During the physical examination, the client's arm remains outstretched after the nurse obtains the pulse and blood pressure, and the nurse must reposition the arm. This client is exhibiting:
A. suggestibility.
B. negativity.
C. waxy flexibility.
D. retardation.
89. A client with borderline personality disorder becomes angry when he is told that today's psychotherapy session with the nurse will be delayed 30 minutes because of an emergency. When the session finally begins, the client expresses anger. Which response by the nurse would be most helpful in dealing with the client's anger?
A. "If it had been your emergency, I would have made the other client wait."
B. "I know it's frustrating to wait. I'm sorry this happened."
C. "You had to wait. Can we talk about how this is making you feel right now?"
D. "I really care about you and I'll never let this happen again."
90. A client begins clozapine (Clozaril) therapy after several other antipsychotic agents fail to relieve her psychotic symptoms. The nurse instructs her to return for weekly white blood cell (WBC) counts to assess for which adverse reaction?
A. Hepatitis
B. Infection
C. Granulocytopenia
D. Systemic dermatitis
91. Which nonantipsychotic medication is used to treat some clients with schizoaffective disorder?
A. phenelzine (Nardil)
B. chlordiazepoxide (Librium)
C. lithium carbonate (Lithane)
D. imipramine (Tofranil)
92. A client diagnosed with schizoaffective disorder is suffering from schizophrenia with elements of which of the following disorders?
A. Personality disorder
B. Mood disorder
C. Thought disorder
D. Amnestic disorder
93. When teaching the family of a client with schizophrenia, the nurse should provide which information?
A. Relapse can be prevented if the client takes the medication.
B. Support is available to help family members meet their own needs.
C. Improvement should occur if the client has a stimulating environment.
D. Stressful family situations can precipitate a relapse in the client.
94. A client is admitted to the psychiatric unit with active psychosis. The physician diagnoses schizophrenia after ruling out several other conditions. Schizophrenia is characterized by:
A. loss of identity and self-esteem.
B. multiple personalities and decreased self-esteem.
C. disturbances in affect, perception, and thought content and form.
D. persistent memory impairment and confusion.
95. The nurse is providing care to a client with a catatonic type of schizophrenia who exhibits extreme negativism. To help the client meet his basic needs, the nurse should:
A. ask the client which activity he would prefer to do first.
B. negotiate a time when the client will perform activities.
C. tell the client specifically and concisely what needs to be done.
D. prepare the client ahead of time for the activity.
96. The nurse is caring for a client who experiences false sensory perceptions with no basis in reality. These perceptions are known as:
A. delusions.
B. hallucinations.
C. loose associations.
D. neologisms.
97. The nurse is aware that antipsychotic medications may cause which of the following adverse effects?
A. Increased production of insulin
B. Lower seizure threshold
C. Increased coagulation time
D. Increased risk of heart failure
98. A client is admitted with a diagnosis of delusions of grandeur. This diagnosis reflects a belief that one is:
A. highly important or famous.
B. being persecuted.
C. connected to events unrelated to oneself.
D. responsible for the evil in the world.
99. A man with a 5-year history of multiple psychiatric admissions is brought to the emergency department by the police. He was found wandering the streets disheveled, shoeless, and confused. Based on his previous medical records and current behavior, he is diagnosed with chronic undifferentiated schizophrenia. The nurse should assign highest priority to which nursing diagnosis?
A. Anxiety
B. Impaired verbal communication
C. Disturbed thought processes
D. Self-care deficient: Dressing/grooming
100. A client's medication order reads, "Thioridazine (Mellaril) 200 mg P.O. q.i.d. and 100 mg P.O. p.r.n." The nurse should:
A. administer the medication as prescribed.
B. question the physician about the order.
C. administer the order for 200 mg P.O. q.i.d. but not for 100 mg P.O. p.r.n.
D. administer the medication as prescribed but observe the client closely for adverse effects.
101. A client is admitted to the psychiatric unit with a diagnosis of borderline personality disorder. The nurse expects the assessment to reveal:
A. unpredictable behavior and intense interpersonal relationships.
B. inability to function as a responsible parent.
C. somatic symptoms.
D. coldness, detachment, and lack of tender feelings.
102. A client with disorganized type schizophrenia has been hospitalized for the past 2 years on a unit for chronic mentally ill clients. The client's behavior is labile and fluctuates from childishness and incoherence to loud yelling to slow but appropriate interaction. The client needs assistance with all activities of daily living. Which behavior is characteristic of disorganized type schizophrenia?
A. Extreme social impairment
B. Suspicious delusions
C. Waxy flexibility
D. Elevated affect
103. The nurse is providing care for a female client with a history of schizophrenia who's experiencing hallucinations. The physician orders 200 mg of haloperidol (Haldol) orally or I.M. every 4 hours as needed. What is the nurse's best action?
A. Administer the haloperidol orally if the client agrees to take it.
B. Call the physician to clarify whether the haloperidol should be given orally or I.M.
C. Call the physician to clarify the order because the dosage is too high.
D. Withhold haloperidol because it may worsen hallucinations.
104. A client receiving haloperidol (Haldol) complains of a stiff jaw and difficulty swallowing. The nurse's first action is to:
A. reassure the client and administer as needed lorazepam (Ativan) I.M.
B. administer as needed dose of benztropine (Cogentin) I.M. as ordered.
C. administer as needed dose of benztropine (Cogentin) by mouth as ordered.
D. administer as needed dose of haloperidol (Haldol) by mouth.
105. A 24-year-old client is experiencing an acute schizophrenic episode. He has vivid hallucinations that are making him agitated. The nurse's best response at this time would be to:
A. take the client's vital signs.
B. explore the content of the hallucinations.
C. tell him his fear is unrealistic.
D. engage the client in reality-oriented activities.
106. Which medication can control the extrapyramidal effects associated with antipsychotic agents?
A. perphenazine (Trilafon)
B. doxepin (Sinequan)
C. amantadine (Symmetrel)
D. clorazepate (Tranxene)
107. A client with paranoid schizophrenia has been experiencing auditory hallucinations for many years. One approach that has proven to be effective for hallucinating clients is to:
A. take an as-needed dose of psychotropic medication whenever they hear voices.
B. practice saying "Go away" or "Stop" when they hear voices.
C. sing loudly to drown out the voices and provide a distraction.
D. go to their room until the voices go away.
108. A dystonic reaction can be caused by which of the following medications?
A. diazepam (Valium)
B. haloperidol (Haldol)
C. amitriptyline (Elavil)
D. clonazepam (Klonopin)
109. While pacing in the hall, a client with paranoid schizophrenia runs to the nurse and says, "Why are you poisoning me? I know you work for central thought control! You can keep my thoughts. Give me back my soul!" How should the nurse respond during the early stage of the therapeutic process?
A. "I'm a nurse. I'm not poisoning you. It's against the nursing code of ethics."
B. "I'm a nurse, and you're a client in the hospital. I'm not going to harm you."
C. "I'm not poisoning you. And how could I possibly steal your soul?"
D. "I sense anger. Are you feeling angry today?"
CLICK HERE FOR ANSWERS AND RATIONALE
Answers and Rationale on Psychotic Disorders
1. A psychotic client reports to the evening nurse that the day nurse put something suspicious in his water with his medication. The nurse replies, "You're worried about your medication?" The nurse's communication is:
A. an example of presenting reality.
B. reinforcing the client's delusions.
C. focusing on emotional content.
D. a nontherapeutic technique called mind reading.
Rationale: The nurse should help the client focus on the emotional content rather than delusional material. Presenting reality isn't helpful because it can lead to confrontation and disengagement. Agreeing with the client and supporting his beliefs are reinforcing delusions. Mind reading isn't therapeutic.
2. A client is admitted to the inpatient unit of the mental health center with a diagnosis of paranoid schizophrenia. He's shouting that the government of France is trying to assassinate him. Which of the following responses is most appropriate?
A. "I think you're wrong. France is a friendly country and an ally of the United States. Their government wouldn't try to kill you."
B. "I find it hard to believe that a foreign government or anyone else is trying to hurt you. You must feel frightened by this."
C. "You're wrong. Nobody is trying to kill you."
D. "A foreign government is trying to kill you? Please tell me more about it."
Rationale: Responses should focus on reality while acknowledging the client's feelings. Arguing with the client or denying his belief isn't therapeutic. Arguing can also inhibit development of a trusting relationship. Continuing to talk about delusions may aggravate the psychosis. Asking the client if a foreign government is trying to kill him may increase his anxiety level and can reinforce his delusions.
3. Propranolol (Inderal) is used in the mental health setting to manage which of the following conditions?
A. Antipsychotic-induced akathisia and anxiety
B. The manic phase of bipolar illness as a mood stabilizer
C. Delusions for clients suffering from schizophrenia
D. Obsessive-compulsive disorder (OCD) to reduce ritualistic behavior
Rationale: Propranolol is a potent beta-adrenergic blocker and produces a sedating effect; therefore, it's used to treat antipsychotic induced akathisia and anxiety. Lithium (Lithobid) is used to stabilize clients with bipolar illness. Antipsychotics are used to treat delusions. Some antidepressants have been effective in treating OCD.
4. A client with borderline personality disorder becomes angry when he is told that today's psychotherapy session with the nurse will be delayed 30 minutes because of an emergency. When the session finally begins, the client expresses anger. Which response by the nurse would be most helpful in dealing with the client's anger?
A. "If it had been your emergency, I would have made the other client wait."
B. "I know it's frustrating to wait. I'm sorry this happened."
C. "You had to wait. Can we talk about how this is making you feel right now?"
D. "I really care about you and I'll never let this happen again."
Rationale: This response may diffuse the client's anger by helping to maintain a therapeutic relationship and addressing the client's feelings. Option A wouldn't address the client's anger. Option B is incorrect because the client with a borderline personality disorder blames others for things that happen, so apologizing reinforces the client's misconceptions. The nurse can't promise that a delay will never occur again, as in option D, because such matters are outside the nurse's control.
5. How soon after chlorpromazine (Thorazine) administration should the nurse expect to see a client's delusional thoughts and hallucinations eliminated
A. Several minutes
B. Several hours
C. Several days
D. Several weeks
Rationale: Although most phenothiazines produce some effects within minutes to hours, their antipsychotic effects may take several weeks to appear.
6. A client receiving haloperidol (Haldol) complains of a stiff jaw and difficulty swallowing. The nurse's first action is to:
A. reassure the client and administer as needed lorazepam (Ativan) I.M.
B. administer as needed dose of benztropine (Cogentin) I.M. as ordered.
C. administer as needed dose of benztropine (Cogentin) by mouth as ordered.
D. administer as needed dose of haloperidol (Haldol) by mouth.
Rationale: The client is most likely suffering from muscle rigidity due to haloperidol. I.M. benztropine should be administered to prevent asphyxia or aspiration. Lorazepam treats anxiety, not extrapyramidal effects. Another dose of haloperidol would increase the severity of the reaction.
7. A client with a diagnosis of paranoid schizophrenia comments to the nurse, "How do I know what is really in those pills?" Which of the following is the best response?
A. Say, "You know it's your medicine."
B. Allow him to open the individual wrappers of the medication.
C. Say, "Don't worry about what is in the pills. It's what is ordered."
D. Ignore the comment because it's probably a joke.
Rationale: Option B is correct because allowing a paranoid client to open his medication can help reduce suspiciousness. Option A is incorrect because the client doesn't know that it's his medication and he's obviously suspicious. Telling the client not to worry or ignoring the comment isn't supportive and doesn't offer reassurance.
8. The nurse is caring for a client with schizophrenia who experiences auditory hallucinations. The client appears to be listening to someone who isn't visible. He gestures, shouts angrily, and stops shouting in mid-sentence. Which nursing intervention is the most appropriate?
A. Approach the client and touch him to get his attention.
B. Encourage the client to go to his room where he'll experience fewer distractions.
C. Acknowledge that the client is hearing voices but make it clear that the nurse doesn't hear these voices.
D. Ask the client to describe what the voices are saying.
Rationale: By acknowledging that the client hears voices, the nurse conveys acceptance of the client. By letting the client know that the nurse doesn't hear the voices, the nurse avoids reinforcing the hallucination. The nurse shouldn't touch the client with schizophrenia without advance warning. The hallucinating client may believe that the touch is a threat or act of aggression and respond violently. Being alone in his room encourages the client to withdraw and may promote more hallucinations. The nurse should provide an activity to distract the client. By asking the client what the voices are saying, the nurse is reinforcing the hallucination. The nurse should focus on the client's feelings, rather than the content of the hallucination.
9. Yesterday, a client with schizophrenia began treatment with haloperidol (Haldol). Today, the nurse notices that the client is holding his head to one side and complaining of neck and jaw spasms. What should the nurse do?
A. Assume that the client is posturing.
B. Tell the client to lie down and relax.
C. Evaluate the client for adverse reactions to haloperidol.
D. Put the client on the list for the physician to see tomorrow
Rationale: An antipsychotic agent, such as haloperidol, can cause muscle spasms in the neck, face, tongue, back, and sometimes legs as well as torticollis (twisted neck position). The nurse should be aware of these adverse reactions and assess for related reactions promptly. Although posturing may occur in clients with schizophrenia, it isn't the same as neck and jaw spasms. Having the client relax can reduce tension-induced muscle stiffness but not drug-induced muscle spasms. When a client develops a new sign or symptom, the nurse should consider an adverse drug reaction as the possible cause and obtain treatment immediately, rather than have the client wait.
10. A client with paranoid schizophrenia has been experiencing auditory hallucinations for many years. One approach that has proven to be effective for hallucinating clients is to:
A. take an as-needed dose of psychotropic medication whenever they hear voices.
B. practice saying "Go away" or "Stop" when they hear voices.
C. sing loudly to drown out the voices and provide a distraction.
D. go to their room until the voices go away.
Rationale: Researchers have found that some clients can learn to control bothersome hallucinations by telling the voices to go away or stop. Taking an as needed dose of psychotropic medication whenever the voices arise may lead to overmedication and put the client at risk for adverse effects. Because the voices aren't likely to go away permanently, the client must learn to deal with the hallucinations without relying on drugs. Although distraction is helpful, singing loudly may upset other clients and would be socially unacceptable after the client is discharged. Hallucinations are most bothersome in a quiet environment when the client is alone, so sending the client to his room would increase, rather than decrease, the hallucinations.
11. A client with catatonic schizophrenia is mute, can't perform activities of daily living, and stares out the window for hours. What is the nurse's first priority?
A. Assist the client with feeding.
B. Assist the client with showering.
C. Reassure the client about safety.
D. Encourage socialization with peers.
Rationale: According to Maslow's hierarchy of needs, the need for food is among the most important. Other needs, in order of decreasing importance, include hygiene, safety, and a sense of belonging.
12. A client tells the nurse that the television newscaster is sending a secret message to her. The nurse suspects the client is experiencing:
A. a delusion.
B. flight of ideas.
C. ideas of reference.
D. a hallucination.
Rationale: Ideas of reference refers to the mistaken belief that neutral stimuli have special meaning to the individual such as the television newscaster sending a message directly to the individual. A delusion is a false belief. Flight of ideas is a speech pattern in which the client skips from one unrelated subject to another. A hallucination is a sensory perception, such as hearing voices and seeing objects, that only the client experiences.
13. The nurse knows that the physician has ordered the liquid form of the drug chlorpromazine (Thorazine) rather than the tablet form because the liquid:
A. has a more predictable onset of action.
B. produces fewer anticholinergic effects.
C. produces fewer drug interactions.
D. has a longer duration of action.
Rationale: A liquid phenothiazine preparation will produce effects in 2 to 4 hours. The onset with tablets is unpredictable.
14. A client who has been hospitalized with disorganized type schizophrenia for 8 years can't complete activities of daily living (ADLs) without staff direction and assistance. The nurse formulates a nursing diagnosis of Self-care deficient: Dressing/grooming related to inability to function without assistance. What is an appropriate goal for this client?
A. "Client will be able to complete ADLs independently within 1 month."
B. "Client will be able to complete ADLs with only verbal encouragement within 1 month."
C. "Client will be able to complete ADLs with assistance in organizing grooming items and clothing within 1 month."
D. "Client will be able to complete ADLs with complete assistance within 1 month."
Rationale: The client's disorganized personality and history of hospitalization have affected the ability to perform self-care activities. Interventions should be directed at helping the client complete ADLs with the assistance of staff members, who can provide needed structure by helping the client select grooming items and clothing. This goal promotes realistic independence. As the client improves and achieves the established goal, the nurse can set new goals that focus on the client completing ADLs with only verbal encouragement and, ultimately, completing them independently. The client's condition doesn't indicate a need for complete assistance, which would only foster dependence.
15. The nurse is planning care for a client admitted to the psychiatric unit with a diagnosis of paranoid schizophrenia. Which nursing diagnosis should receive the highest priority?
A. Risk for violence toward self or others
B. Imbalanced nutrition: Less than body requirements
C. Ineffective family coping
D. Impaired verbal communication
Rationale: Because of such factors as suspiciousness, anxiety, and hallucinations, the client with paranoid schizophrenia is at risk for violence toward himself or others. The other options are also appropriate nursing diagnoses but should be addressed after the safety of the client and those around him is established.
16. The nurse is preparing for the discharge of a client who has been hospitalized for paranoid schizophrenia. The client's husband expresses concern over whether his wife will continue to take her daily prescribed medication. The nurse should inform him that:
A. his concern is valid but his wife is an adult and has the right to make her own decisions.
B. he can easily mix the medication in his wife's food if she stops taking it.
C. his wife can be given a long-acting medication that is administered every 1 to 4 weeks.
D. his wife knows she must take her medication as prescribed to avoid future hospitalizations.
Rationale: Long-acting psychotropic drugs can be administered by depot injection every 1 to 4 weeks. These agents are useful for noncompliant clients because the client receives the injection at the outpatient clinic. A client has the right to refuse medication, but this issue isn't the focus of discussion at this time. Medication should never be hidden in food or drink to trick the client into taking it; besides destroying the client's trust, doing so would place the client at risk for overmedication or undermedication because the amount administered is hard to determine. Assuming the client knows she must take the medication to avoid future hospitalizations would be unrealistic.
17. Benztropine (Cogentin) is used to treat the extrapyramidal effects induced by antipsychotics. This drug exerts its effect by:
A. decreasing the anxiety causing muscle rigidity.
B. blocking the cholinergic activity in the central nervous system (CNS).
C. increasing the level of acetylcholine in the CNS.
D. increasing norepinephrine in the CNS.
Rationale: Option B is the action of Cogentin. Anxiety doesn't cause extrapyramidal effects. Overactivity of acetylcholine and lower levels of dopamine are the causes of extrapyramidal effects. Benztropine doesn't increase norepinephrine in the CNS.
18. A client is admitted to the inpatient unit of the mental health center with a diagnosis of paranoid schizophrenia. He's shouting that the government of France is trying to assassinate him. Which of the following responses is most appropriate?
A. "I think you're wrong. France is a friendly country and an ally of the United States. Their government wouldn't try to kill you."
B. "I find it hard to believe that a foreign government or anyone else is trying to hurt you. You must feel frightened by this."
C. "You're wrong. Nobody is trying to kill you."
D. "A foreign government is trying to kill you? Please tell me more about it."
Rationale: Responses should focus on reality while acknowledging the client's feelings. Arguing with the client or denying his belief isn't therapeutic. Arguing can also inhibit development of a trusting relationship. Continuing to talk about delusions may aggravate the psychosis. Asking the client if a foreign government is trying to kill him may increase his anxiety level and can reinforce his delusions.
19. A dopamine receptor agonist such as bromocriptine (Parlodel) relieves muscle rigidity caused by antipsychotic medication by:
A. blocking dopamine receptors in the central nervous system (CNS).
B. blocking acetylcholine in the CNS.
C. activating norepinephrine in the CNS.
D. activating dopamine receptors in the CNS.
Rationale: Extrapyramidal effects and the muscle rigidity induced by antipsychotic medications are caused by a low level of dopamine. Dopamine receptor agonists stimulate dopamine receptors and thereby reduce rigidity. They don't affect norepinephrine or acetylcholine.
20. Most antipsychotic medications exert which of following effects on the central nervous system (CNS)?
A. Stimulate the CNS by blocking postsynaptic dopamine, norepinephrine, and serotonin receptors.
B. Sedate the CNS by stimulating serotonin at the synaptic cleft.
C. Depress the CNS by blocking the postsynaptic transmission of dopamine, serotonin, and norepinephrine.
D. Depress the CNS by stimulating the release of acetylcholine.
Rationale: The exact mechanism of antipsychotic medication action is unknown, but appear to depress the CNS by blocking the transmission of three neurotransmitters: dopamine, serotonin, and norepinephrine. They don't sedate the CNS by stimulating serotonin, and they don't stimulate neurotransmitter action or acetylcholine release.
21. A client is admitted to the psychiatric unit of a local hospital with chronic undifferentiated schizophrenia. During the next several days, the client is seen laughing, yelling, and talking to herself. This behavior is characteristic of:
A. delusion.
B. looseness of association.
C. illusion.
D. hallucination.
Rationale: Auditory hallucination, in which one hears voices when no external stimuli exist, is common in schizophrenic clients. Such behaviors as laughing, yelling, and talking to oneself suggest such a hallucination. Delusions, also common in schizophrenia, are false beliefs or ideas that arise without external stimuli. Clients with schizophrenia may exhibit looseness of association, a pattern of thinking and communicating in which ideas aren't clearly linked to one another. Illusion is a less severe perceptual disturbance in which the client misinterprets actual external stimuli. Illusions are rarely associated with schizophrenia.
22. Which of the following medications would the nurse expect the physician to order to reverse a dystonic reaction?
A. prochlorperazine (Compazine)
B. diphenhydramine (Benadryl)
C. haloperidol (Haldol)
D. midazolam (Versed)
Rationale: Diphenhydramine, 25 to 50 mg I.M. or I.V., would quickly reverse this condition. Prochlorperazine and haloperidol are both capable of causing dystonia, not reversing it. Midazolam would make this client drowsy.
23. A schizophrenic client states, "I hear the voice of King Tut." Which response by the nurse would be most therapeutic?
A. "I don't hear the voice, but I know you hear what sounds like a voice."
B. "You shouldn't focus on that voice."
C. "Don't worry about the voice as long as it doesn't belong to anyone real."
D. "King Tut has been dead for years."
Rationale: This response states reality about the client's hallucination. The other options are judgmental, flippant, or dismissive.
24. A psychotic client reports to the evening nurse that the day nurse put something suspicious in his water with his medication. The nurse replies, "You're worried about your medication?" The nurse's communication is:
A. an example of presenting reality.
B. reinforcing the client's delusions.
C. focusing on emotional content.
D. a nontherapeutic technique called mind reading.
Rationale: The nurse should help the client focus on the emotional content rather than delusional material. Presenting reality isn't helpful because it can lead to confrontation and disengagement. Agreeing with the client and supporting his beliefs are reinforcing delusions. Mind reading isn't therapeutic.
25. The nurse is caring for a client with schizophrenia who experiences auditory hallucinations. The client appears to be listening to someone who isn't visible. He gestures, shouts angrily, and stops shouting in mid-sentence. Which nursing intervention is the most appropriate?
A. Approach the client and touch him to get his attention.
B. Encourage the client to go to his room where he'll experience fewer distractions.
C. Acknowledge that the client is hearing voices but make it clear that the nurse doesn't hear these voices.
D. Ask the client to describe what the voices are saying
Rationale: By acknowledging that the client hears voices, the nurse conveys acceptance of the client. By letting the client know that the nurse doesn't hear the voices, the nurse avoids reinforcing the hallucination. The nurse shouldn't touch the client with schizophrenia without advance warning. The hallucinating client may believe that the touch is a threat or act of aggression and respond violently. Being alone in his room encourages the client to withdraw and may promote more hallucinations. The nurse should provide an activity to distract the client. By asking the client what the voices are saying, the nurse is reinforcing the hallucination. The nurse should focus on the client's feelings, rather than the content of the hallucination.
26. A client has been receiving chlorpromazine (Thorazine), an antipsychotic, to treat his psychosis. Which findings should alert the nurse that the client is experiencing pseudoparkinsonism?
A. Restlessness, difficulty sitting still, and pacing
B. Involuntary rolling of the eyes
C. Tremors, shuffling gait, and masklike face
D. Extremity and neck spasms, facial grimacing, and jerky movements
Rationale: Pseudoparkinsonism may appear 1 to 5 days after starting an antipsychotic and may also include drooling, rigidity, and "pill rolling." Akathisia may occur several weeks after starting antipsychotic therapy and consists of restlessness, difficulty sitting still, and fidgeting. An oculogyric crisis is recognized by uncontrollable rolling back of the eyes and, along with dystonia, should be considered an emergency. Dystonia may occur minutes to hours after receiving an antipsychotic and may include extremity and neck spasms, jerky muscle movements, and facial grimacing.
27. For several years, a client with chronic schizophrenia has received 10 mg of fluphenazine hydrochloride (Prolixin) by mouth four times per day. Now the client has a temperature of 102° F (38.9° C), a heart rate of 120 beats/minute, a respiratory rate of 20 breaths/minute, and a blood pressure of 210/140 mm Hg. Because the client also is confused and incontinent, the nurse suspects malignant neuroleptic syndrome. What steps should the nurse take?
A. Give the next dose of fluphenazine, call the physician, and monitor vital signs.
B. Withhold the next dose of fluphenazine, call the physician, and monitor vital signs.
C. Give the next dose of fluphenazine and restrict the client to the room to decrease stimulation.
D. Withhold the next dose of fluphenazine, administer an antipyretic agent, and increase the client's fluid intake.
Rationale: Malignant neuroleptic syndrome is a dangerous adverse effect of neuroleptic drugs such as fluphenazine. The nurse should withhold the next dose, notify the physician, and continue to monitor vital signs. Although an antipyretic agent may be used to reduce fever, increased fluid intake is contraindicated because it may increase the client's fluid volume further, raising blood pressure even higher.
28. A schizophrenic client with delusions tells the nurse, "There is a man wearing a red coat who's out to get me." The client exhibits increasing anxiety when focusing on the delusions. Which of the following would be the best response?
A. "This subject seems to be troubling you. Let's walk to the activity room."
B. "Describe the man who's out to get you. What does he look like?"
C. "There is no reason to be afraid of that man. This hospital is very secure."
D. "There is no need to be concerned with a man who isn't even real."
Rationale: This remark distracts the client from the delusion by engaging the client in a less threatening or more comforting activity at the first sign of anxiety. The nurse should reinforce reality and discourage the false belief. The other options focus on the content of the delusion rather than the meaning, feeling, or intent that it provokes.
29. Important teaching for women in their childbearing years who are receiving antipsychotic medications includes which of the following?
A. Occurrence of increased libido due to medication adverse effects
B. Increased incidence of dysmenorrhea while taking the drug
C. Continuing previous use of contraception during periods of amenorrhea
D. Instruction that amenorrhea is irreversible
Rationale: Women may experience amenorrhea, which is reversible, while taking antipsychotics. Amenorrhea doesn't indicate cessation of ovulation; therefore, the client can still become pregnant. The client should be instructed to continue contraceptive use even when experiencing amenorrhea. Dysmenorrhea isn't an adverse effect of antipsychotics, and libido generally decreases because of the depressant effect.
30. A client is admitted to a psychiatric facility with a diagnosis of chronic schizophrenia. The history indicates that the client has been taking neuroleptic medication for many years. Assessment reveals unusual movements of the tongue, neck, and arms. Which condition should the nurse suspect?
A. Tardive dyskinesia
B. Dystonia
C. Neuroleptic malignant syndrome
D. Akathisia
Rationale: Unusual movements of the tongue, neck, and arms suggest tardive dyskinesia, an adverse reaction to neuroleptic medication. Dystonia is characterized by cramps and rigidity of the tongue, face, neck, and back muscles. Neuroleptic malignant syndrome causes rigidity, fever, hypertension, and diaphoresis. Akathisia causes restlessness, anxiety, and jitteriness.
31. What medication would probably be ordered for the acutely aggressive schizophrenic client?
A. chlorpromazine (Thorazine)
B. haloperidol (Haldol)
C. lithium carbonate (Lithonate)
D. amitriptyline (Elavil)
Rationale: Haloperidol administered I.M. or I.V. is the drug of choice for acute aggressive psychotic behavior. Chlorpromazine is also an antipsychotic drug; however, it causes more pronounced sedation than haloperidol. Lithium carbonate is useful in bipolar or manic disorder, and amitriptyline is used for depression.
32. A client is admitted with a diagnosis of schizotypal personality disorder. Which signs would this client exhibit during social situations?
A. Aggressive behavior
B. Paranoid thoughts
C. Emotional affect
D. Independence needs
Rationale: Clients with schizotypal personality disorder experience excessive social anxiety that can lead to paranoid thoughts. Aggressive behavior is uncommon, although these clients may experience agitation with anxiety. Their behavior is emotionally cold with a flattened affect, regardless of the situation. These clients demonstrate a reduced capacity for close or dependent relationships.
33. During the initial interview, a client with schizophrenia suddenly turns to the empty chair beside him and whispers, "Now just leave. I told you to stay home. There isn't enough work here for both of us!" What is the nurse's best initial response?
A. "When people are under stress, they may see things or hear things that others don't. Is that what just happened?"
B. "I'm having a difficult time hearing you. Please look at me when you talk."
C. "There is no one else in the room. What are you doing?"
D. "Who are you talking to? Are you hallucinating?"
Rationale: This response makes the client feel that experiencing hallucinations is acceptable and promotes an open, therapeutic relationship. Directing the client to look at the nurse wouldn't address the obvious issue of the hallucination. Confrontational approaches, such as in options C and D, are likely to elicit an uninformative or negative response.
34. The definition of nihilistic delusions is:
A. a false belief about the functioning of the body.
B. belief that the body is deformed or defective in a specific way.
C. false ideas about the self, others, or the world
D. the inability to carry out motor activities.
Rationale: Nihilistic delusions are false ideas about the self, others, or the world. Somatic delusions involve a false belief about the functioning of the body. Body dysmorphic disorder is characterized by a belief that the body is deformed or defective in a specific way. Apraxia is the inability to carry out motor activities.
35. A client who's taking antipsychotic medication develops a very high temperature, severe muscle rigidity, tachycardia, and rapid deterioration in mental status. The nurse suspects what complication of antipsychotic therapy?
A. Agranulocytosis
B. Extrapyramidal effects
C. Anticholinergic effects
D. Neuroleptic malignant syndrome (NMS)
Rationale: A rare but potentially fatal condition of antipsychotic medication is called NMS. It generally starts with an elevated temperature and severe extrapyramidal effects. Agranulocytosis is a blood disorder. Anticholinergic effects include blurred vision, drowsiness, and dry mouth. Symptoms of extrapyramidal effects include tremors, restlessness, muscle spasms, and pseudoparkinsonism.
36. The nurse formulates a nursing diagnosis of Impaired social interaction related to disorganized thinking for a client with schizotypal personality disorder. Based on this nursing diagnosis, which nursing intervention takes highest priority?
A. Helping the client to participate in social interactions
B. Establishing a one-on-one relationship with the client
C. Exploring the effects of the client's behavior on social interactions
D. Developing a schedule for the client's participation in social interactions
Rationale: By establishing a one-on-one relationship, the nurse helps the client learn how to interact with people in new situations. The other options are appropriate but should take place only after the nurse-client relationship is established.
37. A client with schizophrenia hears a voice telling him he is evil and must die. The nurse understands that the client is experiencing:
A. a delusion.
B. flight of ideas.
C. ideas of reference.
D. a hallucination.
Rationale: A hallucination is a sensory perception, such as hearing voices and seeing objects, that only the client experiences. A delusion is a false belief. Flight of ideas refers to a speech pattern in which the client skips from one unrelated subject to another. Ideas of reference refers to the mistaken belief that someone or something outside the client is controlling the client's ideas or behavior.
38. A client with delusional thinking shows a lack of interest in eating at meal times. She states that she is unworthy of eating and that her children will die if she eats. Which nursing action would be most appropriate for this client?
A. Telling the client that she may become sick and die unless she eats
B. Paying special attention to the client's rituals and emotions associated with meals
C. Restricting the client's access to food except at specified meal and snack times
D. Encouraging the client to express her feelings at meal times
Rationale: Restricting access to food except at specified times prevents the client from eating when she feels anxious, guilty, or depressed; this, in turn, decreases the association between these emotions and food. Telling the client she may become sick or die may reinforce her behavior because illness or death may be her goal. Paying special attention to rituals and emotions associated with meals also would reinforce undesirable behavior. Encouraging the client to express feelings at meal times would increase the association between emotions and food; instead, the nurse should encourage her to express feelings at other times.
39. Which of the following groups of characteristics would the nurse expect to see in the client with schizophrenia?
A. Loose associations, grandiose delusions, and auditory hallucinations
B. Periods of hyperactivity and irritability alternating with depression
C. Delusions of jealousy and persecution, paranoia, and mistrust
D. Sadness, apathy, feelings of worthlessness, anorexia, and weight loss
Rationale: Loose associations, grandiose delusions, and auditory hallucinations are all characteristic of the classic schizophrenic client. These clients aren't able to care for their physical appearance. They frequently hear voices telling them to do something either to themselves or to others. Additionally, they verbally ramble from one topic to the next. Periods of hyperactivity and irritability alternating with depression are characteristic of bipolar or manic disease. Delusions of jealousy and persecution, paranoia, and mistrust are characteristics of paranoid disorders. Sadness, apathy, feelings of worthlessness, anorexia, and weight loss are characteristics of depression.
40. The nurse must administer a medication to reverse or prevent Parkinson-type symptoms in a client receiving an antipsychotic. The medication the client will likely receive is:
A. Benztropine (Cogentin).
B. diphenhydramine (Benadryl).
C. propranolol (Inderal).
D. haloperidol (Haldol).
Rationale: Benztropine, trihexyphenidyl, or amantadine are prescribed for a client with Parkinson-type symptoms. Diphenhydramine provides rapid relief for dystonia. Propranolol relieves akathisia. Haloperidol can cause Parkinson-type symptoms.
41. A client is receiving haloperidol (Haldol) to reduce psychotic symptoms. As he watches television with other clients, the nurse notes that he has trouble sitting still. He seems restless, constantly moving his hands and feet and changing position. When the nurse asks what is wrong, he says he feels jittery. How should the nurse manage this situation?
A. Ask the client to sit still or leave the room because he is distracting the other clients.
B. Ask the client if he is nervous or anxious about something.
C. Give an as needed dose of a prescribed anticholinergic agent to control akathisia.
D. Administer an as needed dose of haloperidol to decrease agitation.
Rationale: Akathisia, characterized by restlessness, is a common but often overlooked adverse reaction to haloperidol and other antipsychotic agents; it may be confused with psychotic agitation. To control akathisia, the nurse should give an as needed dose of a prescribed anticholinergic agent. The client can't control the movements, so asking him to sit still would be pointless. Asking him to leave the room wouldn't address the underlying cause of the problem. Encouraging him to talk about the symptoms wouldn't stop them from occurring. Giving more antipsychotic medication would worsen akathisia.
42. A man is brought to the hospital by his wife, who states that for the past week her husband has refused all meals and accused her of trying to poison him. During the initial interview, the client's speech, only partly comprehensible, reveals that his thoughts are controlled by delusions that he is possessed by the devil. The physician diagnoses paranoid schizophrenia. Schizophrenia is best described as a disorder characterized by:
A. disturbed relationships related to an inability to communicate and think clearly.
B. severe mood swings and periods of low to high activity.
C. multiple personalities, one of which is more destructive than the others.
D. auditory and tactile hallucinations.
Rationale: Schizophrenia is best described as one of a group of psychotic reactions characterized by disturbed relationships with others and an inability to communicate and think clearly. Schizophrenic thoughts, feelings, and behavior commonly are evidenced by withdrawal, fluctuating moods, disordered thinking, and regressive tendencies. Severe mood swings and periods of low to high activity are typical of bipolar disorder. Multiple personality, sometimes confused with schizophrenia, is a dissociative personality disorder, not a psychotic illness. Many schizophrenic clients have auditory hallucinations; tactile hallucinations are more common in organic or toxic disorders
43. A client has a history of chronic undifferentiated schizophrenia. Because she has a history of noncompliance with antipsychotic therapy, she'll receive fluphenazine decanoate (Prolixin Decanoate) injections every 4 weeks. Before discharge, what should the nurse include in her teaching plan?
A. Asking the physician for droperidol (Inapsine) to control any extrapyramidal symptoms that occur
B. Sitting up for a few minutes before standing to minimize orthostatic hypotension
C. Notifying the physician if her thoughts don't normalize within 1 week
D. Expecting symptoms of tardive dyskinesia to occur and to be transient
Rationale: The nurse should teach the client how to manage common adverse reactions, such as orthostatic hypotension and anticholinergic effects. Antipsychotic effects of the drug may take several weeks to appear. Droperidol increases the risk of extrapyramidal effects when given in conjunction with phenothiazines such as fluphenazine. Tardive dyskinesia is a possible adverse reaction and should be reported immediately
44. A client with chronic schizophrenia who takes neuroleptic medication is admitted to the psychiatric unit. Nursing assessment reveals rigidity, fever, hypertension, and diaphoresis. These findings suggest which life-threatening reaction:
A. tardive dyskinesia.
B. dystonia.
C. neuroleptic malignant syndrome.
D. akathisia.
Rationale: The client's signs and symptoms suggest neuroleptic malignant syndrome, a life-threatening reaction to neuroleptic medication that requires immediate treatment. Tardive dyskinesia causes involuntary movements of the tongue, mouth, facial muscles, and arm and leg muscles. Dystonia is characterized by cramps and rigidity of the tongue, face, neck, and back muscles. Akathisia causes restlessness, anxiety, and jitteriness.
45. While looking out the window, a client with schizophrenia remarks, "That school across the street has creatures in it that are waiting for me." Which of the following terms best describes what the creatures represent?
A. Anxiety attack
B. Projection
C. Hallucination
D. Delusion
Rationale: A delusion is a false belief based on a misrepresentation of a real event or experience. Although anxiety can increase delusional responses, it isn't considered the primary symptom. Projection is falsely attributing to another person one's own unacceptable feelings. Hallucinations, which characterize most psychoses, are perceptual disorders of the five senses; the client may see, taste, feel, smell, or hear something in the absence of external stimulation
46. A client with schizophrenia tells the nurse, "My intestines are rotted from the worms chewing on them." This statement indicates a:
A. delusion of persecution.
B. delusion of grandeur.
C. somatic delusion.
D. jealous delusion.
Rationale: Somatic delusions focus on bodily functions or systems and commonly include delusions about foul odor emissions, insect infestations, internal parasites, and misshapen parts. Delusions of persecution are morbid beliefs that one is being mistreated and harassed by unidentified enemies. Delusions of grandeur are gross exaggerations of one's importance, wealth, power, or talents. Jealous delusions are delusions that one's spouse or lover is unfaithful.
47. During the assessment stage, a client with schizophrenia leaves his arm in the air after the nurse has taken his blood pressure. His action shows evidence of:
A. somatic delusions.
B. waxy flexibility.
C. neologisms.
D. nihilistic delusions.
Rationale: The correct answer is waxy flexibility, which is defined as retaining any position that the body has been placed in. Somatic delusions involve a false belief about the functioning of the body. Neologisms are invented meaningless words. Nihilistic delusions are false ideas about self, others, or the world.
48. A client with paranoid type schizophrenia becomes angry and tells the nurse to leave him alone. The nurse should
A. tell him that she'll leave for now but will return soon.
B. ask him if it's okay if she sits quietly with him.
C. ask him why he wants to be left alone.
D. tell him that she won't let anything happen to him
Rationale: If the client tells the nurse to leave, the nurse should leave but let the client know that she'll return so that he doesn't feel abandoned. Not heeding the client's request can agitate him further. Also, challenging the client isn't therapeutic and may increase his anger. False reassurance isn't warranted in this situation
49. Nursing care for a client with schizophrenia must be based on valid psychiatric and nursing theories. The nurse's interpersonal communication with the client and specific nursing interventions must be:
A. clearly identified with boundaries and specifically defined roles.
B. warm and nonthreatening.
C. centered on clearly defined limits and expression of empathy.
D. flexible enough for the nurse to adjust the plan of care as the situation warrants.
Rationale: A flexible plan of care is needed for any client who behaves in a suspicious, withdrawn, or regressed manner or who has a thought disorder. Because such a client communicates at different levels and is in control of himself at various times, the nurse must be able to adjust nursing care as the situation warrants. The nurse's role should be clear; however, the boundaries or limits of this role should be flexible enough to meet client needs. Because a client with schizophrenia fears closeness and affection, a warm approach may be too threatening. Expressing empathy is important, but centering interventions on clearly defined limits is impossible because the client's situation may change without warning.
50. When discharging a client after treatment for a dystonic reaction, the emergency department nurse must ensure that the client understands which of the following?
A. Results of treatment are rapid and dramatic but may not last.
B. Although uncomfortable, this reaction isn't serious.
C. The client shouldn't buy drugs on the street.
D. The client must take benztropine (Cogentin) as prescribed to prevent a return of symptoms.
Rationale: An oral anticholinergic agent such as benztropine (Cogentin) is commonly prescribed to control and prevent the return of symptoms. Dystonic reactions are typically acute and reversible. Dystonic reactions can be life-threatening when airway patency is compromised. Lecturing the client about buying drugs on the street isn't appropriate
51. The nurse is caring for a client with schizophrenia. Which of the following outcomes is the least desirable?
A. The client spends more time by himself.
B. The client doesn't engage in delusional thinking.
C. The client doesn't harm himself or others.
D. The client demonstrates the ability to meet his own self-care needs.
Rationale: The client with schizophrenia is commonly socially isolated and withdrawn; therefore, having the client spend more time by himself wouldn't be a desirable outcome. Rather, a desirable outcome would specify that the client spend more time with other clients and staff on the unit. Delusions are false personal beliefs. Reducing or eliminating delusional thinking using talking therapy and antipsychotic medications would be a desirable outcome. Protecting the client and others from harm is a desirable client outcome achieved by close observation, removing any dangerous objects, and administering medications. Because the client with schizophrenia may have difficulty meeting his or her own self-care needs, fostering the ability to perform self-care independently is a desirable client outcome.
52. The nurse formulates a nursing diagnosis of Impaired verbal communication for a client with schizotypal personality disorder. Based on this nursing diagnosis, which nursing intervention is most appropriate?
A. Helping the client to participate in social interactions
B. Establishing a one-on-one relationship with the client
C. Establishing alternative forms of communication
D. Allowing the client to decide when he wants to participate in verbal communication with the nurse
Rationale: By establishing a one-on-one relationship, the nurse helps the client learn how to interact with people in new situations. The other options are appropriate but should take place only after the nurse-client relationship is established.
53. Since admission 4 days ago, a client has refused to take a shower, stating, "There are poison crystals hidden in the showerhead. They'll kill me if I take a shower." Which nursing action is most appropriate?
A. Dismantling the showerhead and showing the client that there is nothing in it
B. Explaining that other clients are complaining about the client's body odor
C. Asking a security officer to assist in giving the client a shower
D. Accepting these fears and allowing the client to take a sponge bath
Rationale: By acknowledging the client's fears, the nurse can arrange to meet the client's hygiene needs in another way. Because these fears are real to the client, providing a demonstration of reality (as in option A) wouldn't be effective at this time. Options B and C would violate the client's rights by shaming or embarrassing the client.
54. Drug therapy with thioridazine (Mellaril) shouldn't exceed a daily dose of 800 mg to prevent which adverse reaction?
A. Hypertension
B. Respiratory arrest
C. Tourette syndrome
D. Retinal pigmentation
Rationale: Retinal pigmentation may occur if the thioridazine dosage exceeds 800 mg per day. The other options don't occur as a result of exceeding this dose.
55. A client with paranoid personality disorder is admitted to a psychiatric facility. Which remark by the nurse would best establish rapport and encourage the client to confide in the nurse?
A. "I get upset once in a while, too."
B. "I know just how you feel. I'd feel the same way in your situation."
C. "I worry, too, when I think people are talking about me."
D. "At times, it's normal not to trust anyone."
Rationale: Sharing a benign, nonthreatening, personal fact or feeling helps the nurse establish rapport and encourages the client to confide in the nurse. The nurse can't know how the client feels. Telling the client otherwise, as in option B, would justify the suspicions of a paranoid client; furthermore, the client relies on the nurse to interpret reality. Option C is incorrect because it focuses on the nurse's feelings, not the client's. Option D wouldn't help establish rapport or encourage the client to confide in the nurse
56. How soon after chlorpromazine (Thorazine) administration should the nurse expect to see a client's delusional thoughts and hallucinations eliminated?
A. Several minutes
B. Several hours
C. Several days
D. Several weeks
Rationale: Although most phenothiazines produce some effects within minutes to hours, their antipsychotic effects may take several weeks to appear.
57. A client is about to be discharged with a prescription for the antipsychotic agent haloperidol (Haldol), 10 mg by mouth twice per day. During a discharge teaching session, the nurse should provide which instruction to the client?
A. Take the medication 1 hour before a meal.
B. Decrease the dosage if signs of illness decrease.
C. Apply a sunscreen before being exposed to the sun.
D. Increase the dosage up to 50 mg twice per day if signs of illness don't decrease.
Rationale: Because haloperidol can cause photosensitivity and precipitate severe sunburn, the nurse should instruct the client to apply a sunscreen before exposure to the sun. The nurse also should teach the client to take haloperidol with meals — not 1 hour before — and should instruct the client not to decrease or increase the dosage unless the physician orders it
58. A client with paranoid schizophrenia repeatedly uses profanity during an activity therapy session. Which response by the nurse would be most appropriate?
A. "Your behavior won't be tolerated. Go to your room immediately."
B. "You're just doing this to get back at me for making you come to therapy."
C. "Your cursing is interrupting the activity. Take time out in your room for 10 minutes."
D. "I'm disappointed in you. You can't control yourself even for a few minutes."
Rationale: The nurse should set limits on client behavior to ensure a comfortable environment for all clients. The nurse should accept hostile or quarrelsome client outbursts within limits without becoming personally offended, as in option A. Option B is incorrect because it implies that the client's actions reflect feelings toward the staff instead of the client's own misery. Judgmental remarks, such as option D, may decrease the client's self-esteem.
59. Which of the following is one of the advantages of the newer antipsychotic medication risperidone (Risperdal)?
A. The absence of anticholinergic effects
B. A lower incidence of extrapyramidal effects
C. Photosensitivity and sedation
D. No incidence of neuroleptic malignant syndrome
Rationale: Risperdal has a lower incidence of extrapyramidal effects than the typical antipsychotics. Risperdal does produce anticholinergic effects and neuroleptic malignant syndrome can occur. Photosensitivity isn't an advantage.
60. The etiology of schizophrenia is best described by:
A. genetics due to a faulty dopamine receptor.
B. environmental factors and poor parenting.
C. structural and neurobiological factors.
D. a combination of biological, psychological, and environmental factors.
Rationale: A reliable genetic marker hasn't been determined for schizophrenia. However, studies of twins and adopted siblings have strongly implicated a genetic predisposition. Since the mid-19th century, excessive dopamine activity in the brain has also been suggested as a causal factor. Communication and the family system have been studied as contributing factors in the development of schizophrenia. Therefore, a combination of biological, psychological, and environmental factors are thought to cause schizophrenia.
61. A client with schizophrenia who receives fluphenazine (Prolixin) develops pseudoparkinsonism and akinesia. What drug would the nurse administer to minimize extrapyramidal symptoms?
A. benztropine (Cogentin)
B. dantrolene (Dantrium)
C. clonazepam (Klonopin)
D. diazepam (Valium)
Rationale: Benztropine is an anticholinergic drug administered to reduce extrapyramidal adverse effects in the client taking antipsychotic drugs. It works by restoring the equilibrium between the neurotransmitters acetylcholine and dopamine in the central nervous system (CNS). Dantrolene, a hydantoin drug that reduces the catabolic processes, is administered to alleviate the symptoms of neuroleptic malignant syndrome, a potentially fatal adverse effect of antipsychotic drugs. Clonazepam, a benzodiazepine drug that depresses the CNS, is administered to control seizure activity. Diazepam, a benzodiazepine drug, is administered to reduce anxiety.
62. A client with a diagnosis of paranoid schizophrenia comments to the nurse, "How do I know what is really in those pills?" Which of the following is the best response?
A. Say, "You know it's your medicine."
B. Allow him to open the individual wrappers of the medication.
C. Say, "Don't worry about what is in the pills. It's what is ordered."
D. Ignore the comment because it's probably a joke.
Rationale: Option B is correct because allowing a paranoid client to open his medication can help reduce suspiciousness. Option A is incorrect because the client doesn't know that it's his medication and he's obviously suspicious. Telling the client not to worry or ignoring the comment isn't supportive and doesn't offer reassurance.
63. A client tells the nurse that people from Mars are going to invade the earth. Which response by the nurse would be most therapeutic?
A. "That must be frightening to you. Can you tell me how you feel about it?"
B. "There are no people living on Mars."
C. "What do you mean when you say they're going to invade the earth?"
D. "I know you believe the earth is going to be invaded, but I don't believe that."
Rationale: This response addresses the client's underlying fears without feeding the delusion. Refuting the client's delusion, as in option B, would increase anxiety and reinforce the delusion. Asking the client to elaborate on the delusion, as in option C, would also reinforce it. Voicing disbelief about the delusion, as in option D, wouldn't help the client deal with underlying fears
64. A client with schizophrenia tells the nurse he hears the voices of his dead parents. To help the client ignore the voices, the nurse should recommend that he:
A. sit in a quiet, dark room and concentrate on the voices.
B. listen to a personal stereo through headphones and sing along with the music.
C. call a friend and discuss the voices and his feelings about them.
D. engage in strenuous exercise.
Rationale: Increasing the amount of auditory stimulation, such as by listening to music through headphones, may make it easier for the client to focus on external sounds and ignore internal sounds from auditory hallucinations. Option A would make it harder for the client to ignore the hallucinations. Talking about the voices, as in option C, would encourage the client to focus on them. Option D is incorrect because exercise alone wouldn't provide enough auditory stimulation to drown out the voices.
65. A client with schizophrenia is receiving antipsychotic medication. Which nursing diagnosis may be appropriate for this client?
A. Ineffective protection related to blood dyscrasias
B. Urinary frequency related to adverse effects of antipsychotic medication
C. Risk for injury related to a severely decreased level of consciousness
D. Risk for injury related to electrolyte disturbances
Rationale: Antipsychotic medications may cause neutropenia and granulocytopenia, life-threatening blood dyscrasias, that warrant a nursing diagnosis of Ineffective protection related to blood dyscrasias. These medications also have anticholinergic effects, such as urine retention, dry mouth, and constipation. Urinary frequency isn't an approved nursing diagnosis. Although antipsychotic medications may cause sedation, they don't severely decrease the level of consciousness, eliminating option C. These drugs don't cause electrolyte disturbances, eliminating option D.
66. A client with persistent, severe schizophrenia has been treated with phenothiazines for the past 17 years. Now the client's speech is garbled as a result of drug-induced rhythmic tongue protrusion. What is another name for this extrapyramidal symptom?
A. Dystonia
B. Akathisia
C. Pseudoparkinsonism
D. Tardive dyskinesia
Rationale: An adverse reaction to phenothiazines, tardive dyskinesia refers to choreiform tongue movements that commonly are irreversible and may interfere with speech. Dystonia refers to involuntary contraction of a muscle group. Akathisia is restlessness or inability to sit still. Pseudoparkinsonism describes a group of symptoms that mimic those of Parkinson's disease.
67. The nurse is assigned to a client with catatonic schizophrenia. Which intervention should the nurse include in the client's plan of care?
A. Meeting all of the client's physical needs
B. Giving the client an opportunity to express concerns
C. Administering lithium carbonate (Lithonate) as prescribed
D. Providing a quiet environment where the client can be alone
Rationale: Because a client with catatonic schizophrenia can't meet physical needs independently, the nurse must provide for all of these needs, including adequate food and fluid intake, exercise, and elimination. This client is incapable of expressing concerns; however, the nurse should try to verbalize the message conveyed by the client's nonverbal behavior. Lithium is used to treat mania, not catatonic schizophrenia. Despite the client's mute, unresponsive state, the nurse should provide nonthreatening stimulation and should spend time with the client, not leave the client alone all the time. Although aware of the environment, the client doesn't interact with it actively; the nurse's support and presence can be reassuring.
68. A client with a history of medication noncompliance is receiving outpatient treatment for chronic undifferentiated schizophrenia. The physician is most likely to prescribe which medication for this client?
A. chlorpromazine (Thorazine)
B. imipramine (Tofranil)
C. lithium carbonate (Lithane)
D. fluphenazine decanoate (Prolixin Decanoate)
Rationale: Fluphenazine decanoate is a long-acting antipsychotic agent given by injection. Because it has a 4-week duration of action, it's commonly prescribed for outpatients with a history of medication noncompliance. Chlorpromazine, also an antipsychotic agent, must be administered daily to maintain adequate plasma levels, which necessitates compliance with the dosage schedule. Imipramine, a tricyclic antidepressant, and lithium carbonate, a mood stabilizer, are rarely used to treat clients with chronic schizophrenia.
69. Propranolol (Inderal) is used in the mental health setting to manage which of the following conditions?
A. Antipsychotic-induced akathisia and anxiety
B. The manic phase of bipolar illness as a mood stabilizer
C. Delusions for clients suffering from schizophrenia
D. Obsessive-compulsive disorder (OCD) to reduce ritualistic behavior
Rationale: Propranolol is a potent beta-adrenergic blocker and produces a sedating effect; therefore, it's used to treat antipsychotic induced akathisia and anxiety. Lithium (Lithobid) is used to stabilize clients with bipolar illness. Antipsychotics are used to treat delusions. Some antidepressants have been effective in treating OCD.
70. Every day for the past 2 weeks, a client with schizophrenia stands up during group therapy and screams, "Get out of here right now! The elevator bombs are going to explode in 3 minutes!" The next time this happens, how should the nurse respond?
A. "Why do you think there is a bomb in the elevator?"
B. "That is the same thing you said in yesterday's session."
C. "I know you think there are bombs in the elevator, but there aren't."
D. "If you have something to say, you must do it according to our group rules."
Rationale: Option C is the most therapeutic response because it orients the client to reality. Options A and B are condescending. Option D sounds punitive and could embarrass the client.
71. A 26-year-old client is admitted to the psychiatric unit with acute onset of schizophrenia. His physician prescribes the phenothiazine chlorpromazine (Thorazine), 100 mg by mouth four times per day. Before administering the drug, the nurse reviews the client's medication history. Concomitant use of which drug is likely to increase the risk of extrapyramidal effects?
A. guanethidine (Ismelin)
B. droperidol (Inapsine)
C. lithium carbonate (Lithonate)
D. alcohol
Rationale: When administered with any phenothiazine, droperidol may increase the risk of extrapyramidal effects. The other options are incorrect
72. A client, age 36, with paranoid schizophrenia believes the room is bugged by the Central Intelligence Agency and that his roommate is a foreign spy. The client has never had a romantic relationship, has no contact with family members, and hasn't been employed in the last 14 years. Based on Erikson's theories, the nurse should recognize that this client is in which stage of psychosocial development?
A. Autonomy versus shame and doubt
B. Generativity versus stagnation
C. Integrity versus despair
D. Trust versus mistrust
Rationale: This client's paranoid ideation indicates difficulty trusting others. The stage of autonomy versus shame and doubt deals with separation, cooperation, and self-control. Generativity versus stagnation is the normal stage for this client's chronologic age. Integrity versus despair is the stage for accepting the positive and negative aspects of one's life, which would be difficult or impossible for this client.
73. During a group therapy session in the psychiatric unit, a client constantly interrupts with impulsive behavior and exaggerated stories that cast her as a hero or princess. She also manipulates the group with attention-seeking behaviors, such as sexual comments and angry outbursts. The nurse realizes that these behaviors are typical of:
A. paranoid personality disorder.
B. avoidant personality disorder.
C. histrionic personality disorder.
D. borderline personality disorder.
Rationale: This client's behaviors are typical of histrionic personality disorder, which is marked by excessive emotionality and attention seeking. The client constantly seeks and demands attention, approval, or praise; may be seductive in behavior, appearance, or conversation; and is uncomfortable except when she is the center of attention. Typically, a client with paranoid personality disorder is suspicious, cold, hostile, and argumentative. Avoidant personality disorder is characterized by anxiety, fear, and social isolation. Borderline personality disorder is characterized by impulsive, unpredictable behavior and unstable, intense interpersonal relationships.
74. The nurse is teaching a psychiatric client about her prescribed drugs, chlorpromazine and benztropine. Why is benztropine administered?
A. To reduce psychotic symptoms
B. To reduce extrapyramidal symptoms
C. To control nausea and vomiting
D. To relieve anxiety
Rationale: Benztropine is an anticholinergic medication, administered to reduce the extrapyramidal adverse effects of chlorpromazine and other antipsychotic medications. Benztropine doesn't reduce psychotic symptoms, relieve anxiety, or control nausea and vomiting.
75. A client is admitted to the psychiatric unit with a tentative diagnosis of psychosis. Her physician prescribes the phenothiazine thioridazine (Mellaril) 50 mg by mouth three times per day. Phenothiazines differ from central nervous system (CNS) depressants in their sedative effects by producing:
A. deeper sleep than CNS depressants.
B. greater sedation than CNS depressants.
C. a calming effect from which the client is easily aroused.
D. more prolonged sedative effects, making the client more difficult to arouse.
Rationale: Shortly after phenothiazine administration, a quieting and calming effect occurs, but the client is easily aroused, alert, and responsive and has good motor coordination.
76. A woman is admitted to the psychiatric emergency department. Her significant other reports that she has difficulty sleeping, has poor judgment, and is incoherent at times. The client's speech is rapid and loose. She reports being a special messenger from the Messiah. She has a history of depressed mood for which she has been taking an antidepressant. The nurse suspects which diagnosis?
A. Schizophrenia
B. Paranoid personality
C. Bipolar illness
D. Obsessive-compulsive disorder (OCD)
Rationale: Bipolar illness is characterized by mood swings from profound depression to elation and euphoria. Delusions of grandeur along with pressured speech are common symptoms of mania. Schizophrenia doesn't exhibit mood swings from depression to euphoria. Paranoia is characterized by unrealistic suspiciousness and is often accompanied by grandiosity. OCD is a preoccupation with rituals and rules.
77. A client with paranoid schizophrenia is admitted to the psychiatric unit of a hospital. Nursing assessment should include careful observation of the client's:
A. thinking, perceiving, and decision-making skills.
B. verbal and nonverbal communication processes.
C. affect and behavior.
D. psychomotor activity.
Rationale: Nursing assessment of a psychotic client should include careful inquiry about and observation of the client's thinking, perceiving, symbolizing, and decision-making skills and abilities. Assessment of such a client typically reveals alterations in thought content and process, perception, affect, and psychomotor behavior; changes in personality, coping, and sense of self; lack of self-motivation; presence of psychosocial stressors; and degeneration of adaptive functioning. Although assessing communication processes, affect, behavior, and psychomotor activity would reveal important information about the client's condition, the nurse should concentrate on determining whether the client is hallucinating by assessing thought processes and decision-making ability.
78. Which information is most important for the nurse to include in a teaching plan for a schizophrenic client taking clozapine (Clozaril)?
A. Monthly blood tests will be necessary.
B. Report a sore throat or fever to the physician immediately.
C. Blood pressure must be monitored for hypertension.
D. Stop the medication when symptoms subside.
Rationale: A sore throat and fever are indications of an infection caused by agranulocytosis, a potentially life-threatening complication of clozapine. Because of the risk of agranulocytosis, white blood cell (WBC) counts are necessary weekly, not monthly. If the WBC count drops below 3,000/μl, the medication must be stopped. Hypotension may occur in clients taking this medication. Warn the client to stand up slowly to avoid dizziness from orthostatic hypotension. The medication should be continued, even when symptoms have been controlled. If the medication must be stopped, it should be slowly tapered over 1 to 2 weeks and only under the supervision of a physician.
79. Important teaching for clients receiving antipsychotic medication such as haloperidol (Haldol) includes which of the following instructions?
A. Use sunscreen because of photosensitivity.
B. Take the antipsychotic medication with food.
C. Have routine blood tests to determine levels of the medication.
D. Abstain from eating aged cheese.
* A and B are both correct in taking HALDOL.
80. Positive symptoms of schizophrenia include which of the following?
A. Hallucinations, delusions, and disorganized thinking
B. Somatic delusions, echolalia, and a flat affect
C. Waxy flexibility, alogia, and apathy
D. Flat affect, avolition, and anhedonia
Rationale: The positive symptoms of schizophrenia are distortions of normal functioning. Option A lists the positive symptoms of schizophrenia. A flat affect, alogia, apathy, avolition, and anhedonia refer to the negative symptoms. Negative symptoms list the diminution or loss of normal function
81. A client with chronic schizophrenia receives 20 mg of fluphenazine decanoate (Prolixin Decanoate) by I.M. injection. Three days later, the client has muscle contractions that contort the neck. This client is exhibiting which extrapyramidal reaction?
A. Dystonia
B. Akinesia
C. Akathisia
D. Tardive dyskinesia
Rationale: Dystonia, a common extrapyramidal reaction to fluphenazine decanoate, manifests as muscle spasms in the tongue, face, neck, back, and sometimes the legs. Akinesia refers to decreased or absent movement; akathisia, to restlessness or inability to sit still; and tardive dyskinesia, to abnormal muscle movements, particularly around the mouth.
82. Hormonal effects of the antipsychotic medications include which of the following?
A. Retrograde ejaculation and gynecomastia
B. Dysmenorrhea and increased vaginal bleeding
C. Polydipsia and dysmenorrhea
D. Akinesia and dysphasia
Rationale: Decreased libido, retrograde ejaculation, and gynecomastia are all hormonal effects that can occur with antipsychotic medications. Reassure the client that the effects can be reversed or that changing medication may be possible. Polydipsia, akinesia, and dysphasia aren't hormonal effects.
83. A client is unable to get out of bed and get dressed unless the nurse prompts every step. This is an example of which behavior?
A. Word salad
B. Tangential
C. Perseveration
D. Avolition
Rationale: Avolition refers to impairment in the ability to initiate goal-directed activity. Word salad is when a group of words are put together in a random fashion without logical connection. Tangential is where a person never gets to the point of the communication. Perseveration is when a person repeats the same word or idea in response to different questions.
84. An agitated and incoherent client, age 29, comes to the emergency department with complaints of visual and auditory hallucinations. The history reveals that the client was hospitalized for paranoid schizophrenia from ages 20 to 21. The physician prescribes haloperidol (Haldol), 5 mg I.M. The nurse understands that this drug is used in this client to treat:
A. dyskinesia.
B. dementia.
C. psychosis.
D. tardive dyskinesia.
Rationale: By treating psychosis, haloperidol, an antipsychotic drug, decreases agitation. Haloperidol is used to treat dyskinesia in clients with Tourette syndrome and to treat dementia in elderly clients. Tardive dyskinesia may occur after prolonged haloperidol use; the client should be monitored for this adverse reaction.
85. Yesterday, a client with schizophrenia began treatment with haloperidol (Haldol). Today, the nurse notices that the client is holding his head to one side and complaining of neck and jaw spasms. What should the nurse do?
A. Assume that the client is posturing.
B. Tell the client to lie down and relax.
C. Evaluate the client for adverse reactions to haloperidol.
D. Put the client on the list for the physician to see tomorrow.
Rationale: An antipsychotic agent, such as haloperidol, can cause muscle spasms in the neck, face, tongue, back, and sometimes legs as well as torticollis (twisted neck position). The nurse should be aware of these adverse reactions and assess for related reactions promptly. Although posturing may occur in clients with schizophrenia, it isn't the same as neck and jaw spasms. Having the client relax can reduce tension-induced muscle stiffness but not drug-induced muscle spasms. When a client develops a new sign or symptom, the nurse should consider an adverse drug reaction as the possible cause and obtain treatment immediately, rather than have the client wait.
86. A client receiving fluphenazine decanoate (Prolixin Decanoate) therapy develops pseudoparkinsonism. The physician is likely to prescribe which drug to control this extrapyramidal effect?
A. phenytoin (Dilantin)
B. amantadine (Symmetrel)
C. benztropine (Cogentin)
D. diphenhydramine (Benadryl)
Rationale: An antiparkinsonian agent, such as amantadine, may be used to control pseudoparkinsonism; diphenhydramine or benztropine may be used to control other extrapyramidal effects. Phenytoin is used to treat seizure activity.
87. Important teaching for a client receiving risperidone (Risperdal) would include advising the client to:
A. double the dose if missed to maintain a therapeutic level.
B. be sure to take the drug with a meal because it's very irritating to the stomach.
C. discontinue the drug if the client reports weight gain.
D. notify the physician if the client notices an increase in bruising.
Rationale: Bruising may indicate blood dyscrasias, so notifying the physician about increased bruising is very important. Don't double the dose. This drug doesn't irritate the stomach, and weight gain isn't a problem.
88. A client is admitted to the psychiatric hospital with a diagnosis of catatonic schizophrenia. During the physical examination, the client's arm remains outstretched after the nurse obtains the pulse and blood pressure, and the nurse must reposition the arm. This client is exhibiting:
A. suggestibility.
B. negativity.
C. waxy flexibility.
D. retardation.
Rationale: Waxy flexibility, the ability to assume and maintain awkward or uncomfortable positions for long periods, is characteristic of catatonic schizophrenia. Clients commonly remain in these awkward positions until someone repositions them. Clients with dependency problems may demonstrate suggestibility, a response pattern in which one easily agrees to the ideas and suggestions of others rather than making independent judgments. Negativity (for example, resistance to being moved or being asked to cooperate) and retardation (slowed movement) also occur in catatonic clients.
89. A client with borderline personality disorder becomes angry when he is told that today's psychotherapy session with the nurse will be delayed 30 minutes because of an emergency. When the session finally begins, the client expresses anger. Which response by the nurse would be most helpful in dealing with the client's anger?
A. "If it had been your emergency, I would have made the other client wait."
B. "I know it's frustrating to wait. I'm sorry this happened."
C. "You had to wait. Can we talk about how this is making you feel right now?"
D. "I really care about you and I'll never let this happen again."
Rationale: This response may diffuse the client's anger by helping to maintain a therapeutic relationship and addressing the client's feelings. Option A wouldn't address the client's anger. Option B is incorrect because the client with a borderline personality disorder blames others for things that happen, so apologizing reinforces the client's misconceptions. The nurse can't promise that a delay will never occur again, as in option D, because such matters are outside the nurse's control.
90. A client begins clozapine (Clozaril) therapy after several other antipsychotic agents fail to relieve her psychotic symptoms. The nurse instructs her to return for weekly white blood cell (WBC) counts to assess for which adverse reaction?
A. Hepatitis
B. Infection
C. Granulocytopenia
D. Systemic dermatitis
Rationale: Clozapine can cause life-threatening neutropenia or granulocytopenia. To detect this adverse reaction, a WBC count should be performed weekly. Hepatitis, infection, and systemic dermatitis aren't adverse reactions of clozapine therapy.
91. Which nonantipsychotic medication is used to treat some clients with schizoaffective disorder?
A. phenelzine (Nardil)
B. chlordiazepoxide (Librium)
C. lithium carbonate (Lithane)
D. imipramine (Tofranil)
Rationale: Lithium carbonate, an antimania drug, is used to treat clients with cyclical schizoaffective disorder, a psychotic disorder once classified under schizophrenia that causes affective symptoms, including maniclike activity. Lithium helps control the affective component of this disorder. Phenelzine is a monoamine oxidase inhibitor prescribed for clients who don't respond to other antidepressant drugs such as imipramine. Chlordiazepoxide, an antianxiety agent, generally is contraindicated in psychotic clients. Imipramine, primarily considered an antidepressant agent, is also used to treat clients with agoraphobia and those undergoing cocaine detoxification.
92. A client diagnosed with schizoaffective disorder is suffering from schizophrenia with elements of which of the following disorders?
A. Personality disorder
B. Mood disorder
C. Thought disorder
D. Amnestic disorder
Rationale: According to the DSM-IV, schizoaffective disorder refers to clients suffering from schizophrenia with elements of a mood disorder, either mania or depression. The prognosis is generally better than for the other types of schizophrenia, but it's worse than the prognosis for a mood disorder alone. Option A is incorrect because personality disorders and psychotic illness aren't listed together on the same axis. Option C is incorrect because schizophrenia is a major thought disorder and the question asks for elements of another disorder. Clients with schizoaffective disorder aren't suffering from schizophrenia and an amnestic disorder.
93. When teaching the family of a client with schizophrenia, the nurse should provide which information?
A. Relapse can be prevented if the client takes the medication.
B. Support is available to help family members meet their own needs.
C. Improvement should occur if the client has a stimulating environment.
D. Stressful family situations can precipitate a relapse in the client.
Rationale: Because family members of a client with schizophrenia face difficult situations and great stress, the nurse should inform them of support services that can help them cope with such problems. The nurse should also teach them that medication can't prevent relapses and that environmental stimuli may precipitate symptoms. Although stress can trigger symptoms, the nurse shouldn't make the family feel responsible for relapses (as in option D).
94. A client is admitted to the psychiatric unit with active psychosis. The physician diagnoses schizophrenia after ruling out several other conditions. Schizophrenia is characterized by:
A. loss of identity and self-esteem.
B. multiple personalities and decreased self-esteem.
C. disturbances in affect, perception, and thought content and form.
D. persistent memory impairment and confusion.
Rationale: The Diagnostic and Statistic Manual of Mental Disorders, 4th edition, defines schizophrenia as a disturbance in multiple psychological processes that affects thought content and form, perception, affect, sense of self, volition, relationship to the external world, and psychomotor behavior. Loss of identity sometimes occurs but is only one characteristic of the disorder. Multiple personalities typify multiple personality disorder, a dissociative personality disorder. Mood disorders are commonly accompanied by increased or decreased self-esteem. Schizophrenia doesn't cause a disturbance in sensorium, although the client may exhibit confusion, disorientation, and memory impairment during the acute phase.
95. The nurse is providing care to a client with a catatonic type of schizophrenia who exhibits extreme negativism. To help the client meet his basic needs, the nurse should:
A. ask the client which activity he would prefer to do first.
B. negotiate a time when the client will perform activities.
C. tell the client specifically and concisely what needs to be done.
D. prepare the client ahead of time for the activity.
Rationale: The client needs to be informed of the activity and when it will be done. Giving the client choices isn't desirable because he can be manipulative or refuse to do anything. Negotiating and preparing the client ahead of time also isn't therapeutic with this type of client because he may not want to perform the activity.
96. The nurse is caring for a client who experiences false sensory perceptions with no basis in reality. These perceptions are known as:
A. delusions.
B. hallucinations.
C. loose associations.
D. neologisms.
Rationale: Hallucinations are visual, auditory, gustatory, tactile, or olfactory perceptions that have no basis in reality. Delusions are false beliefs, rather than perceptions, that the client accepts as real. Loose associations are rapid shifts among unrelated ideas. Neologisms are bizarre words that have meaning only to the client.
97. The nurse is aware that antipsychotic medications may cause which of the following adverse effects?
A. Increased production of insulin
B. Lower seizure threshold
C. Increased coagulation time
D. Increased risk of heart failure
Rationale: Antipsychotic medications exert an effect on brain neurotransmitters that lowers the seizure threshold and can, therefore, increase the risk of seizure activity. Antipsychotics don't affect insulin production or coagulation time. Heart failure isn't an adverse effect of antipsychotic agents
98. A client is admitted with a diagnosis of delusions of grandeur. This diagnosis reflects a belief that one is:
A. highly important or famous.
B. being persecuted.
C. connected to events unrelated to oneself.
D. responsible for the evil in the world.
Rationale: A delusion of grandeur is a false belief that one is highly important or famous. A delusion of persecution is a false belief that one is being persecuted. A delusion of reference is a false belief that one is connected to events unrelated to oneself or a belief that one is responsible for the evil in the world.
99. A man with a 5-year history of multiple psychiatric admissions is brought to the emergency department by the police. He was found wandering the streets disheveled, shoeless, and confused. Based on his previous medical records and current behavior, he is diagnosed with chronic undifferentiated schizophrenia. The nurse should assign highest priority to which nursing diagnosis?
A. Anxiety
B. Impaired verbal communication
C. Disturbed thought processes
D. Self-care deficient: Dressing/grooming
Rationale: For this client, the highest-priority nursing diagnosis is Anxiety (severe to panic-level), manifested by the client's extreme withdrawal and attempt to protect himself from the environment. The nurse must act immediately to reduce anxiety and protect the client and others from possible injury. Impaired verbal communication, manifested by noncommunicativeness; Disturbed thought processes, evidenced by inability to understand the situation; and Self-care deficient: Dressing/grooming, evidenced by a disheveled appearance, are appropriate nursing diagnoses but aren't the highest priority
100. A client's medication order reads, "Thioridazine (Mellaril) 200 mg P.O. q.i.d. and 100 mg P.O. p.r.n." The nurse should:
A. administer the medication as prescribed.
B. question the physician about the order.
C. administer the order for 200 mg P.O. q.i.d. but not for 100 mg P.O. p.r.n.
D. administer the medication as prescribed but observe the client closely for adverse effects.
Rationale: The nurse must question this order immediately. Thioridazine (Mellaril) has an absolute dosage ceiling of 800 mg/day. Any dosage above this level places the client at high risk for toxic pigmentary retinopathy, which can't be reversed. As written, the order allows for administering more than the maximum 800 mg/day; it should be corrected immediately, before the client's health is jeopardized.
101. A client is admitted to the psychiatric unit with a diagnosis of borderline personality disorder. The nurse expects the assessment to reveal:
A. unpredictable behavior and intense interpersonal relationships.
B. inability to function as a responsible parent.
C. somatic symptoms.
D. coldness, detachment, and lack of tender feelings.
Rationale: A client with borderline personality disorder displays a pervasive pattern of unpredictable behavior, mood, and self-image. Interpersonal relationships may be intense and unstable and behavior may be inappropriate and impulsive. Although the client's impaired ability to form relationships may affect parenting skills, inability to function as a responsible parent is more typical of antisocial personality disorder. Somatic symptoms characterize avoidant personality disorder. Coldness, detachment, and lack of tender feelings typify schizoid and schizotypal personality disorders.
102. A client with disorganized type schizophrenia has been hospitalized for the past 2 years on a unit for chronic mentally ill clients. The client's behavior is labile and fluctuates from childishness and incoherence to loud yelling to slow but appropriate interaction. The client needs assistance with all activities of daily living. Which behavior is characteristic of disorganized type schizophrenia?
A. Extreme social impairment
B. Suspicious delusions
C. Waxy flexibility
D. Elevated affect
Rationale: Disorganized type schizophrenia (formerly called hebephrenia) is characterized by extreme social impairment, marked inappropriate affect, silliness, grimacing, posturing, and fragmented delusions and hallucinations. A client with a paranoid disorder typically exhibits suspicious delusions, such as a belief that evil forces are after him. Waxy flexibility, a condition in which the client's limbs remain fixed in uncomfortable positions for long periods, characterizes catatonic schizophrenia. Elevated affect is associated with schizoaffective disorder.
103. The nurse is providing care for a female client with a history of schizophrenia who's experiencing hallucinations. The physician orders 200 mg of haloperidol (Haldol) orally or I.M. every 4 hours as needed. What is the nurse's best action?
A. Administer the haloperidol orally if the client agrees to take it.
B. Call the physician to clarify whether the haloperidol should be given orally or I.M.
C. Call the physician to clarify the order because the dosage is too high.
D. Withhold haloperidol because it may worsen hallucinations.
Rationale: The dosage is too high (normal dosage ranges from 5 to 10 mg daily). Options A and B may lead to an overdose. Option D is incorrect because haloperidol helps with symptoms of hallucinations.
104. A client receiving haloperidol (Haldol) complains of a stiff jaw and difficulty swallowing. The nurse's first action is to:
A. reassure the client and administer as needed lorazepam (Ativan) I.M.
B. administer as needed dose of benztropine (Cogentin) I.M. as ordered.
C. administer as needed dose of benztropine (Cogentin) by mouth as ordered.
D. administer as needed dose of haloperidol (Haldol) by mouth.
Rationale: The client is most likely suffering from muscle rigidity due to haloperidol. I.M. benztropine should be administered to prevent asphyxia or aspiration. Lorazepam treats anxiety, not extrapyramidal effects. Another dose of haloperidol would increase the severity of the reaction.
105. A 24-year-old client is experiencing an acute schizophrenic episode. He has vivid hallucinations that are making him agitated. The nurse's best response at this time would be to:
A. take the client's vital signs.
B. explore the content of the hallucinations.
C. tell him his fear is unrealistic.
D. engage the client in reality-oriented activities.
Rationale: Exploring the content of the hallucinations will help the nurse understand the client's perspective on the situation. The client shouldn't be touched, such as in taking vital signs, without telling him exactly what is going to happen. Debating with the client about his emotions isn't therapeutic. When the client is calm, engage him in reality-based activities.
106. Which medication can control the extrapyramidal effects associated with antipsychotic agents?
A. perphenazine (Trilafon)
B. doxepin (Sinequan)
C. amantadine (Symmetrel)
D. clorazepate (Tranxene)
Rationale: Amantadine is an anticholinergic drug used to relieve drug-induced extrapyramidal adverse effects, such as muscle weakness, involuntary muscle movement, pseudoparkinsonism, and tardive dyskinesia. Other anticholinergic agents used to control extrapyramidal reactions include benztropine mesylate (Cogentin), trihexyphenidyl (Artane), biperiden (Akineton), and diphenhydramine (Benadryl). Perphenazine is an antipsychotic agent; doxepin, an antidepressant; and chlorazepate, an antianxiety agent. Because these medications have no anticholinergic or neurotransmitter effects, they don't alleviate extrapyramidal reactions.
107. A client with paranoid schizophrenia has been experiencing auditory hallucinations for many years. One approach that has proven to be effective for hallucinating clients is to:
A. take an as-needed dose of psychotropic medication whenever they hear voices.
B. practice saying "Go away" or "Stop" when they hear voices.
C. sing loudly to drown out the voices and provide a distraction.
D. go to their room until the voices go away.
Rationale: Researchers have found that some clients can learn to control bothersome hallucinations by telling the voices to go away or stop. Taking an as needed dose of psychotropic medication whenever the voices arise may lead to overmedication and put the client at risk for adverse effects. Because the voices aren't likely to go away permanently, the client must learn to deal with the hallucinations without relying on drugs. Although distraction is helpful, singing loudly may upset other clients and would be socially unacceptable after the client is discharged. Hallucinations are most bothersome in a quiet environment when the client is alone, so sending the client to his room would increase, rather than decrease, the hallucinations.
108. A dystonic reaction can be caused by which of the following medications?
A. diazepam (Valium)
B. haloperidol (Haldol)
C. amitriptyline (Elavil)
D. clonazepam (Klonopin)
Rationale: Haloperidol is a phenothiazine and is capable of causing dystonic reactions. Diazepam and clonazepam are benzodiazepines, and amitriptyline is a tricyclic antidepressant. Benzodiazepines don't cause dystonic reactions; however, they can cause drowsiness, lethargy, and hypotension. Tricyclic antidepressants rarely cause severe dystonic reactions; however, they can cause a decreased level of consciousness, tachycardia, dry mouth, and dilated pupils.
109. While pacing in the hall, a client with paranoid schizophrenia runs to the nurse and says, "Why are you poisoning me? I know you work for central thought control! You can keep my thoughts. Give me back my soul!" How should the nurse respond during the early stage of the therapeutic process?
A. "I'm a nurse. I'm not poisoning you. It's against the nursing code of ethics."
B. "I'm a nurse, and you're a client in the hospital. I'm not going to harm you."
C. "I'm not poisoning you. And how could I possibly steal your soul?"
D. "I sense anger. Are you feeling angry today?"
Rationale: The nurse should directly orient a delusional client to reality, especially to place and person. Options A and C may encourage further delusions by denying poisoning and offering information related to the delusion. Validating the client's feelings, as in option D, occurs during a later stage in the therapeutic process.
ANSWERS AND RATIONALE
1. 60 YEAR OLD POST CVA PATIENT IS TAKING TPA FOR HIS DISEASE, THE NURSE UNDERSTANDS THAT THIS IS AN EXAMPLE OF WHAT LEVEL OF PREVENTION?
C. TERTIARY : THE CLIENT ALREADY HAD STROKE, TPA STANDS FOR TRANSPLASMINOGEN ACTIVATOR WHICH ARE THROMBOLYTICS, DISSOLVING CLOTS FORMED IN THE VESSELS OF THE BRAIN. WE ARE JUST PREVENTING COMPLICATIONS HERE.
2. A FEMALE CLIENT UNDERGOES YEARLY MAMMOGRAPHY. THIS IS A TYPE OF WHAT LEVEL OF PREVENTION?
B. SECONDARY : THE CLIENT IS NEVER SICK OF ANYTHING BUT WE ARE DETECTING THE POSSIBILITY BY GIVING YEARLY MAMMOGRAPHY. REMEMBER THAT ALL KINDS OF TESTS, CASE FINDINGS AND TREATMENT BELONGS TO THE SECONDARY LEVEL OF PREVENTION.
3. A DIABETIC PATIENT WAS AMPUTATED FOLLOWING AN UNEXPECTED NECROSIS ON THE RIGHT LEG, HE SUSTAINED AND UNDERGONE BKA. HE THEN UNDERWENT THERAPY ON HOW TO USE HIS NEW PROSTHETIC LEG. THIS IS A TYPE OF WHAT LEVEL OF PREVENTION?
C. TERTIARY : TERTIARY PREVENTION INVOLVES REHABILITATION. CLIENT IS NOW BEING ASSISTED TO PERFORM ADLS AT HIS OPTIMUM FUNCTIONING. REMEMBER THAT ALL KINDS OF REHABILITATORY AND PALLIATIVE MANAGEMENT IS INCLUDED IN TERTIARY PREVENTION.
4. AS A CARE PROVIDER, THE NURSE SHOULD DO FIRST:
D. EARLY RECOGNITION OF THE CLIENT’S NEEDS. : WE ARE TALKING ABOUT WHAT SHOULD THE NURSE DO FIRST. ASSESSMENT INVOLVES EARLY RECOGNITION OF CLIENTS NEEDS. A,B,C ARE ALL INVOLVE IN THE INTERVENTION PHASE OF THE NURSING PROCESS.
5. AS A MANAGER, THE NURSE SHOULD:
D. WORKS TOGETHER WITH THE TEAM. : AS A NURSE MANAGER, YOU SHOULD BE ABLE TO WORK WITH THE TEAM. A,B,C ARE NOT SPECIFIC OF A NURSE MANAGER. THEY CAN BE DONE BY AN ORDINARY R.N.
6. THE NURSE SHOWS A PATIENT ADVOCATE ROLE WHEN
A. DEFEND THE PATIENTS RIGHT : AN ADVOCATE ROLE IS SHOWN WHEN THE NURSE DEFENDS THE RIGHTS OF THE CLIENT. INTERCEDING IN BEHALF OF THE PATIENT SHOULD NOT BE DONE BY A NURSE. COUNTER TRANSFERENCE CAN DEVELOP IN THAT CASE AND WE SHOULD AVOID THAT. ONLY THE FAMILY AND THE HEALTH ATTORNEY OF THE PATIENT CAN INTERCEDE OR SPEAK FOR THE PATIENT.
7. WHICH IS THE FOLLOWING IS THE MOST APPROPRIATE DURING THE ORIENTATION PHASE ?
D. ESTABLISHMENT OF REGULAR MEETING OF SCHEDULES : ORIENTATION PHASE IS SYNONYMOUS WITH CONTRACT ESTABLISHMENT. HERE, THE NURSE WILL ESTABLISH REGULAR MEETING OF SCHEDULE, AGREEMENTS AND GIVING THE CLIENT INFORMATION THAT THERE IS A TERMINATION. LETTER A AND B ASSESSES THE CLIENT’S COPING SKILLS, WHICH IS IN THE WORKING PHASE AND SO IS LETTER B. IN WORKING PHASE, THE NURSE ASSESSES THE COPING SKILLS OF THE CLIENT AND FORMULATE PLANS AND INTERVENTION TO CORRECT DEFICIENCIES. ALTHOUGH ASSESSMENT IS ALSO MADE IN THE ORIENTATION PHASE, COPING SKILLS ARE ASSESSED IN THE WORKING PHASE.
8. PREPARING THE CLIENT FOR THE TERMINATION PHASE BEGINS :
C. WORKING : TELLING THE CLIENT THAT THERE IS A TERMINATION PHASE SHOULD BE IN THE ORIENTATION PHASE, HOWEVER, IN PREPARING THE CLIENT FOR THE TERMINATION, IT SHOULD BE DONE IN THE WORKING PHASE. THE NURSE WILL START TO LESSEN THE NUMBER OF MEETINGS TO PREVENT DEVELOPMENT OF TRANSFERENCE OR COUNTER TRANSFERENCE.
9. A HELPING RELATIONSHIP IS A PROCESS CHARACTERIZED BY :
C. GROWTH FACILITATING : IN PSYCHIATRIC NURSING, THE EPITOME OF ALL NURSING GOAL SHOULD FOCUS ON FACILITATING GROWTH OF THE CLIENT.
10. DURING THE NURSE PATIENT INTERACTION, THE NURSE ASSESS THE FF: TO DETERMINE THE PATIENTS COPING STRATEGY :
D. HOW DOES YOUR PROBLEM AFFECT YOUR LIFE? : THIS IS THE ONLY QUESTION THAT DETERMINES THE EFFECTS OF THE PROBLEM ON THE CLIENT AND THE WAYS SHE IS DEALING WITH IT. LETTER A CAN ONLY BE ANSWERED BY FINE AND CLOSE FURTHER COMMUNICATION. B IS UNRELATED TO COPING STRATEGIES. LETTER C, ASKING THE CLIENT WHAT DO YOU THINK CAN HELP YOU RIGHT NOW IS INAPPROPRIATE FOR THE NURSE TO ASK. THE CLIENT IS IN THE HOSPITAL BECAUSE SHE NEEDS HELP. IF SHE KNOWS SOMETHING THAT CAN HELP HER WITH HER PROBLEM SHE SHOULDN’T BE THERE.
11. AS A COUNSELOR, THE NURSE PERFORMS WHICH OF THE FF: TASK?
A. ENCOURAGE CLIENT TO EXPRESS FEELINGS AND CONCERNS : A COUNSELOR IS MUCH MORE OF A LISTENER THAN A SPEAKER. SHE ENCOURAGE THE CLIENT TO EXPRESS FEELINGS AND CONCERNS AS TO FORMULATE NECESSARY RESPONSE AND FACILITATE A CHANNEL TO EXPRESS ANGER, DISAPPOINTMENTS AND FRUSTRATIONS.
12. FREUD STRESSES OUT THAT THE EGO
A. DISTINGUISHES BETWEEN THINGS IN THE MIND AND THINGS IN THE REALITY. : THE EGO IS RESPONSIBLE FOR DISTINGUISHING WHAT IS REAL AND WHAT IS NOT. IT IS THE ONE THAT BALANCES THE ID AND SUPER EGO. B AND D IS A CHARACTERISTIC OF THE SUPER EGO WHICH IS THE CONTROLLER OF INSTINCTS AND DRIVES AND SERVE AS OUR CONSCIENCE OR THE MORAL ARM. THE ID IS OUR DRIVES AND INSTINCTS THAT IS MEDIATED BY THE EGO AND CONTROLLED BY THE SUPER EGO.
13. A 16 YEAR OLD CHILD IS HOSPITALIZED, ACCORDING TO ERIK ERIKSON, WHAT IS AN APPROPRIATE INTERVENTION?
A. TELL THE FRIENDS TO VISIT THE CHILD : THE CHILD IS 16 YEARS OLD, IN THE STAGE OF IDENTITY VS. ROLE CONFUSION. THE MOST SIGNIFICANT PERSONS IN THIS GROUP ARE THE PEERS. B REFERS TO CHILDREN IN THE SCHOOL AGE WHILE C REFERS TO THE YOUNG ADULTHOOD STAGE OF INTIMACY VS. ISOLATION. THE CHILD IS NOT DYING AND THE SITUATION DID NOT EVEN TALK ABOUT THE CHILD’S BELIEF THEREFORE, CALLING THE PRIEST IS UNNECESSARY.
14. NMS IS CHARACTERIZED BY :
C. HYPERTENSION, HYPERTHERMIA, DIAPHORESIS. : NEUROLEPTIC MALIGNANT SYNDROME IS A SIDE EFFECT OF NEUROLEPTICS. THIS IS CHARACTERIZED BY FEVER, INCREASE IN BLOOD PRESSURE AND WARM, DIAPHORETIC SKIN.
15. WHICH OF THE FOLLOWING DRUGS NEEDS A WBC LEVEL CHECKED REGULARLY?
B. CLOZARIL : CLOZAPINE IS A DREADED AYPICAL ANTIPSYCHOTIC BECAUSE IT CAUSES SEVERE BONE MARROW DEPRESSION, AGRANULOCYTOSIS, INFECTION AND SORE THROAT. WBC COUNT IS IMPORTANT TO ASSESS IF THE CLIENTS IMMUNE FUNCTION IS SEVERELY IMPAIRED. THE FIRST PRESENTING SIGN OF AGRANULOCYTOSIS IS SORE THROAT.
SITUATION : ANGELO, AN 18 YEAR OLD OUT OF SCHOOL YOUTH WAS CAUGHT SHOPLIFTING IN A DEPARTMENT STORE. HE HAS HISTORY OF BEING QUARRELSOME AND INVOLVING PHYSICAL FIGHT WITH HIS FRIENDS. HE HAS BEEN OUT OF JAIL FOR THE PAST TWO YEARS
16. INITIALLY, THE NURSE IDENTIFIES WHICH OF THE FF: NURSING DIAGNOSIS:
B. IMPAIRED SOCIAL INTERACTION : THERE IS NO SUCH NURSING DIAGNOSIS AS A , LOOKING AT C AND D, THEY ARE MUCH MORE COMPATIBLE TO SCHIZOPHRENIA WHICH IS NOT A CHARACTERISTIC OF AN ANTI SOCIAL P.D WHICH IS SHOWN IN THE SITUATION. REMEMBER THAT PERSONALITY DISORDER IS FAR FROM PSYCHOSES. WHEN CLIENT EXHIBITS ALTERED THOUGHT PROCESS OR SENSORY ALTERATION, IT IS NOT ANYMORE A PERSONALITY DISORDER BUT RATHER, A SIGN AND SYMPTOM OF PSYCHOSES.
17. WHICH OF THE FF: IS NOT A CHARACTERISTIC OF PD?
B. LOSS OF COGNITIVE FUNCTIONING : AS I SAID, SYMPTOMS OF PD WILL NEVER SHOW ALTERATION IN COGNITIVE FUNCTIONING. THEY ARE MUCH MORE OF SOCIAL DISTURBANCES RATHER THAN PSYCHOLOGICAL.
18. THE MOST EFFECTIVE TREATMENT MODALITY FOR PERSONS IF ANTI SOCIAL PD IS
C. BEHAVIOR THERAPY : THE PROBLEM OF THE PATIENT IS HIS BEHAVIOR. A IS DONE FOR PATIENT WHO HAS INSOMNIA OR SEVERE ANXIETY. B IS A THERAPY THAT PROMOTES GROWTH BY PROVIDING A CONTACT, EITHER A PERSON OR AN ENVIRONMENT WHO WILL FACILITATE THE GROWTH OF AN INDIVIDUAL. IT IS A HUMANISTIC PSYCHOTHERAPEUTIC MODEL APPROACH. D IS DONE ON CLIENTS WHO ARE IN CRISIS LIKE TRAUMA, POST TRAUMATIC DISORDERS, RAPED OR ACCIDENTS.
19. WHICH OF THE FOLLOWING IS NOT AN EXAMPLE OF ALTERATION OF PERCEPTION?
B. FLIGHT OF IDEAS : FLIGHT OF IDEAS IS A CONDITION IN WHICH PATIENT TALKS CONTINUOUSLY AND THEN SWITCHING TO UNRELATED TOPIC. AN EXAMPLE IS “ ANG GANDA NG BULAKLAK NA ITO NO BUDEK? ROSE ITO HINDI BA? KILALA MO BA SI JACK YUNG BOYFRIEND NI ROSE? GRABE YUNG BARKO NO ANG LAKI LAKI TAPOS LUMUBOG LANG. DAPAT SANA NAG SEAMAN AKO EH, GUSTO KASI NG NANAY KO. “. LOOSE ASSOCIATION IS SOMEWHAT SIMILAR BUT THE SWITCH IN TOPIC IS MORE OBVIOUS AND COMPLETELY UNRELATED. EXAMPLE “ ANG CUTE NUNG RABBIT, PAANO SI PAUL KASI TANGA EH, PAPAPATAY KO YAN KAY ALBERT. ANG GANDA NUNG BAG NA BINIGAY NI JENNY, TANGA NGA LANG YUNG ASWANG DUN SA KANTO. PERO BAKIT KA BA ANDITO? WALA AKONG PAGKAIN, PENGE AKO KOTSE AAKYAT AKO EVEREST.”
A,C,D ARE ALL ALTERATION IN PERCEPTION. A REFERS TO A PERSON THINKING THAT EVERYONE IS TALKING ABOUT HIM. C AND D ARE ALL SENSORY ALTERATIONS. THE DIFFERENCE IS THAT, IN HALLUCINATION, THERE IS NO NEED FOR A STIMULI. IN ILLUSION, A STIMULI [ A PHONE CORD ] IS MISTAKENLY IDENTIFIED BY THE CLIENT AS SOMETHING ELSE [ SNAKE ]
20. THE TYPE OF ANXIETY THAT LEADS TO PERSONALITY DISORGANIZATION IS :
D. PANIC : PANIC IS THE ONLY LEVEL OF ANXIETY THAT LEADS TO PERSONALITY DISORGANIZATION.
21. A CLIENT IS ADMITTED TO THE HOSPITAL. TWELVE HOURS LATER THE NURSE OBSERVES HAND TREMORS, HYPEREXICITABILITY, TACHYCARDIA, DIAPHORESIS AND HYPERTENSION. THE NURSE SUSPECTS ALCOHOL WITHDRAWAL. THE NURSE SHOULD ASK THE CLIENT:
A. AT WHAT TIME WAS YOUR LAST DRINK TAKEN? : THIS QUESTION WILL GIVE THE NURSE IDEA WHEN WILL THE WITHDRAWAL OCCUR. WITHDRAWAL OCCURS 5 TO 10 HOURS AFTER THE LAST INTAKE OF ALCOHOL. THIS IS A CRUCIAL AND MORTALITY IS VERY HIGH DURING THIS PERIOD. CLIENT WILL UNDERGO DELIRIUM TREMENS, SEIZURES AND DEATH IF NOT RECOGNIZE EARLIER BY THE NURSE. B IS VERY JUDGMENTAL, C IS NON SPECIFIC, WHETHER IT IS A BEER OR A WINE IT IS STILL ALCOHOL AND HAS THE SAME EFFECTS. D IS A VALUABLE QUESTION TO DETERMINE THE CHRONIC EFFECTS OF ALCOHOL INGESTION BUT ASKING LETTER A CAN BROADEN THE LINE BETWEEN LIFE AND DEATH.
22. CLIENT WITH A HISTORY OF SCHIZOPHRENIA HAS BEEN ADMITTED FOR SUICIDAL IDEATION. THE CLIENT STATES "GOD IS TELLING ME TO KILL MYSELF RIGHT NOW." THE NURSE'S BEST RESPONSE IS:
A. I UNDERSTAND THAT GOD’S VOICE ARE REAL TO YOU, BUT I DON’T HEAR ANYTHING. I WILL STAY WITH YOU. : THE NURSE SHOULD FIRST ACKNOWLEDGE THAT THE VOICES ARE REAL TO THE PATIENT AND THEN, PRESENT REALITY BY TELLING THE PATIENT THAT YOU DO NOT HEAR ANYTHING. THE THIRD PART OF THE NURSING INTERVENTION IN HALLUCINATION IS LESSENING THE STIMULI BY EITHER STAYING WITH THE PATIENT OR REMOVING THE PATIENT FROM A HIGHLY STIMULATING PLACE.
TELLING THE CLIENT THAT THE VOICES IS PART OF HIS ILLNESS IS NOT THERAPEUTIC. PEOPLE WITH SCHIZOPHRENIA DO NOT THINK THAT THEY ARE ILL. LETTER C AND D DISREGARDS THE CLIENT’S CONCERN AND THEREFORE, NOT THERAPEUTIC.
23. IN ASSESSING A CLIENT'S SUICIDE POTENTIAL, WHICH STATEMENT BY THE CLIENT WOULD GIVE THE NURSE THE HIGHEST CAUSE FOR CONCERN?
C. I’VE THOUGHT ABOUT TAKING PILLS AND ALCOHOL TILL I PASS OUT : THIS IS THE ONLY STATEMENT OF THE CLIENT THAT CONTAINS A SPECIFIC AND TECHNICAL PLAN. B,D ARE ALL INDICATIVE OF SUICIDAL IDEATION BUT IT CONTAINS NO SPECIFIC PLANS TO CARRY OUT THE OBJECTIVE. LETTER A ADMITS THE CLIENT THINKS OF HURTING HIMSELF, BUT NOT DOING IT BECAUSE IT SCARES HIM, THEREFORE, IT IS NOT INDICATIVE OF SUICIDAL IDEATION.
24. A CLIENT WITH PARANOID SCHIZOPHRENIA HAS PERSECUTORY DELUSIONS AND AUDITORY HALLUCINATIONS AND IS EXTREMELY AGITATED. HE HAS BEEN GIVEN A PRN DOSE OF THORAZINE IM. WHICH OF THE FOLLOWING WOULD INDICATE TO THE NURSE THAT THE MEDICATION IS HAVING THE DESIRED EFFECT?
C. STOPS PACING AND SITS WITH THE NURSE : THORAZINE IS A NEUROLEPTIC. DESIRED EFFECT EVOLVE ON CONTROLLING THE CLIENT’S PSYCHOSES. LETTER A IS THE SIDE EFFECT OF THE DRUG, WHICH IS NOT DESIRED. B AND D INDICATES THAT THE DRUG IS NOT EFFECTIVE IN CONTROLLING THE CLIENT’S AGITATION, RESTLESSNESS AND DISORDERS OF PERCEPTION.
25. A CLIENT WHO WAS WANDERING AIMLESSLY AROUND THE STREETS ACTING INAPPROPRIATELY AND APPEARED DISHEVELED AND UNKEMPT WAS ADMITTED TO A PSYCHIATRIC UNIT AND IS EXPERIENCING AUDITORY AND VISUAL HALLUCINATIONS. THE NURSE WOULD DEVELOP A PLAN OF CARE BASED ON:
C. SCHIZOPHRENIA : WHEN DISORDERS OF PERCEPTION AND THOUGHTS CAME IN, THE ONLY FEASIBLE DIAGNOSIS A DOCTOR CAN MAKE IS AMONG THE CHOICES IS SCHIZOPHRENIA. A,B AND D CAN OCCUR IN NORMAL INDIVIDUALS WITHOUT ALTERING THEIR PERCEPTIONS. SCHIZOPHRENIA IS CHARACTERIZED BY DISORDERS OF THOUGHTS, HALLUCINATION, DELUSION, ILLUSION AND DISORGANIZATION.
26. A DECISION IS MADE TO NOT HOSPITALIZE A CLIENT WITH OBSESSIVE-COMPULSIVE DISORDER. OF THE FOLLOWING ABILITIES THE CLIENT HAS DEMONSTRATED, THE ONE THAT PROBABLY MOST INFLUENCED THE DECISION NOT TO HOSPITALIZE HIM IS HIS ABILITY TO:
C. PERFORM ACTIVITIES OF DAILY LIVING : IF A CLIENT CAN DO ADLS , THERE IS NO REASON FOR THAT CLIENT TO BE HOSPITALIZED.
27. A CLIENT IS ADMITTED TO THE INPATIENT PSYCHIATRIC UNIT. HE IS UNSHAVEN, HAS BODY ODOR, AND HAS SPOTS ON HIS SHIRT AND PANTS. HE MOVES SLOWLY, GAZES AT THE FLOOR, AND HAS A FLAT AFFECT. THE NURSE'S HIGHEST PRIORITY IN ASSESSING THE CLIENT ON ADMISSION WOULD BE TO ASK HIM:
B. IF HE IS THINKING ABOUT HURTING HIMSELF : THE CLIENT SHOWS TYPICAL SIGN AND SYMPTOMS OF DEPRESSION. MOVING SLOWLY, GAZES ON THE FLOOR, BLANK STARES AND SHOWING FLAT AFFECT. THE HIGHEST PRIORITY AMONG DEPRESSED CLIENT IS ASSESSING ANY SUICIDE PLANS OR IDEATION FOR THE NURSE TO ESTABLISH A NO SUICIDE CONTRACT EARLY ON OR, IN ANY CASE CLIENT DO NOT PARTICIPATE IN A NO SUICIDE CONTRACT, A 24 HOUR CONTINUOUS MONITORING IS ESTABLISHED.
28. THE NURSE SHOULD KNOW THAT THE NORMAL THERAPEUTIC LEVEL OF LITHIUM IS :
A. .6 TO .12 MEQ/L : ACCORDING TO BRUNNER AND SUDDARTHS MS NURSING, THE NORMAL THERAPEUTIC LEVEL OF LITHIUM IS .6 TO 1.2 MEQ/L. SOME BOOKS WILL SAY .5 TO 1.5 MEQ/L.
29. THE PATIENT COMPLAINT OF VOMITING, DIARRHEA AND RESTLESSNESS AFTER TAKING LITHANE. THE NURSE’S INITIAL INTERVENTION IS :
A. RECOGNIZE THAT THIS IS A SIGN OF TOXICITY AND WITHHOLD THE NEXT MEDICATION. : THE NURSE SHOULD RECOGNIZE THAT THIS IS AN EARLY S/S OF LITHIUM TOXICITY. TAKING THE CLIENTS VITAL SIGNS WILL NOT CONFIRM DIARRHEA, VOMITING OR RESTLESSNESS. NOTIFYING THE PHYSICIAN IS UNNECESSARY AT THIS POINT AND THE PHYSICIAN WILL LIKELY TO WITHHOLD THE MEDICATION.
30. THE CLIENT IS TAKING TOFRANIL. THE NURSE SHOULD CLOSELY MONITOR THE PATIENT FOR :
C. INCREASE INTRA OCULAR PRESSURE : TOFRANIL IS A NEUROLEPTIC. IT IS WELL KNOWN THAT THIS IS THE ANTIPSYCHOTIC THAT INCREASES THE IOP AND CONTRAINDICATED IN PATIENTS WITH GLAUCOMA. HYPERTENSION IS NOT SPECIFIC WITH TOFRANIL. ALL NEUROLEPTICS CAN CAUSE NMS OR THE NEUROLEPTIC MALIGNANT SYNDROME.
31. A CLIENT WAS HOSPITALIZED WITH MAJOR DEPRESSION WITH SUICIDAL IDEATION FOR 1 WEEK. HE IS TAKING VENLAFAXINE (EFFEXOR), 75 MG THREE TIMES A DAY, AND IS PLANNING TO RETURN TO WORK. THE NURSE ASKS THE CLIENT IF HE IS EXPERIENCING THOUGHTS OF SELF-HARM. THE CLIENT RESPONDS, "I HARDLY THINK ABOUT IT ANYMORE AND WOULDN'T DO ANYTHING TO HURT MYSELF." THE NURSE JUDGES:
C. THE DEPRESSION TO BE IMPROVING AND THE SUICIDAL IDEATION TO BE LESSENING. : TOO OBVIOUS, NO NEED TO RATIONALIZE.
32. THE CLIENT IS TAKING SERTRALINE (ZOLOFT), 50 MG Q AM. THE NURSE INCLUDES WHICH OF THE FOLLOWING IN THE TEACHING PLAN ABOUT ZOLOFT?
A. ZOLOFT CAUSES ERECTILE DYSFUNCTION IN MEN : WHEN YOU TAKE ZOLOFT, MAG ZOZOLOFT KA NALANG SA BUHAY. BECAUSE IT CAUSES ERECTILE DYSFUNTION AND DECREASE LIBIDO. LETTER B AND C ARE SPECIFIC OF TCAS. ZOLOFT WILL EXERT ITS EFFECTS AS EARLY AS 1 WEEK.
33. AFTER 3 DAYS OF TAKING HALOPERIDOL, THE CLIENT SHOWS AN INABILITY TO SIT STILL, IS RESTLESS AND FIDGETY, AND PACES AROUND THE UNIT. OF THE FOLLOWING EXTRAPYRAMIDAL ADVERSE REACTIONS, THE CLIENT IS SHOWING SIGNS OF:
B. AKATHISIA : THE CLIENT SHOWS SIGN OF MOTOR RESTLESSNESS, WHICH IS SPECIFIC FOR AKATHISIA OR MAKATI SYA.
34. AFTER 10 DAYS OF LITHIUM THERAPY, THE CLIENT'S LITHIUM LEVEL IS 1.0 MEQ/L. THE NURSE KNOWS THAT THIS VALUE INDICATES WHICH OF THE FOLLOWING?
B. AN ANTICIPATED THERAPEUTIC BLOOD LEVEL OF THE DRUG.
35. WHEN CARING FOR A CLIENT RECEIVING HALOPERIDOL (HALDOL), THE NURSE WOULD ASSESS FOR WHICH OF THE FOLLOWING?
B. EXTRAPYRAMIDAL SYMPTOMS : HALDOL IS A NEUROLEPTIC, SPECIFIC TO THESE NEUROLEPTICS ARE THE EPS. THE CLIENT WILL LIKELY BE HYPOTENSIVE THAN HYPERTENSIVE BECAUSE NEUROLEPTICS CAUSES POSTURAL HYPOTENSION, THE CLIENT WILL COMPLAINT OF DRY MOUTH DUE TO ITS ANTICHOLINERGIC PROPERTIES. DIZZINESS AND DROWSINESS ARE SIDE EFFECTS OF NEUROLEPTICS BUT NOT OVERSEDATION.
36. A CLIENT IS BROUGHT TO THE HOSPITAL’S EMERGENCY ROOM BY A FRIEND, WHO STATES, "I GUESS HE HAD SOME BAD JUNK (HEROIN) TODAY." IN ASSESSING THE CLIENT, THE NURSE WOULD LIKELY FIND WHICH OF THE FOLLOWING SYMPTOMS?
C. DECREASED RESPIRATIONS, CONSTRICTED PUPILS, AND PALLOR. : HEROIN IS A NARCOTIC. TOGETHER WITH MORPHINE, MEPERIDINE, CODEINE AND OPIODS, THEY ARE DEPRESSANTS AND WILL CAUSE DECREASE RESPIRATION, CONSTRICTED PUPILS AND PALLOR DUE TO VASOCONSTRICTION.
37. THE CLIENT HAS BEEN TAKING THE MONOAMINE OXIDASE INHIBITOR (MAOI) PHENELZINE (NARDIL), 10 MG BID. THE PHYSICIAN ORDERS A SELECTIVE SEROTONIN REUPTAKE INHIBITOR (SSRI), PAROXETINE (PAXIL), 20 MG GIVEN EVERY MORNING. THE NURSE:
B. QUESTIONS THE PHYSICIAN ABOUT THE ORDER : 2 ANTI DEPRESSANTS CANNOT BE GIVEN AT THE SAME TIME UNLESS THE OTHER ONE IS TAPERED WHILE THE OTHER ONE IS GIVEN GRADUALLY.
38. WHICH OF THE FOLLOWING CLIENT STATEMENTS ABOUT CLOZAPINE (CLOZARIL) INDICATES THAT THE CLIENT NEEDS ADDITIONAL TEACHING?
D. "I NEED TO CALL MY DOCTOR WHENEVER I NOTICE THAT I HAVE A FEVER OR SORE THROAT." : CLOZAPINE CAUSES AGRANULOCYTOSIS AND BONE MARROW DEPRESSION. EARLY S/S INCLUDES FEVER AND SORE THROAT. THE MEDICATION IS TO BE WITHHELD THIS TIME OR THE PATIENT MIGHT DEVELOP SEVERE INFECTION LEADING TO DEATH.
39. A CLIENT HAS BEEN TAKING LITHIUM CARBONATE (LITHANE) FOR HYPERACTIVITY, AS PRESCRIBED BY HIS PHYSICIAN. WHILE THE CLIENT IS TAKING THIS DRUG, THE NURSE SHOULD ENSURE THAT HE HAS AN ADEQUATE INTAKE OF:
A. SODIUM : THE LEVELS OF LITHIUM IN THE BODY ARE DEPENDENT ON SODIUM. THE HIGHER THE SODIUM, THE LOWER THE LEVELS OF LITHIUM. CLIENTS SHOULD HAVE AN ADEQUATE INTAKE OF SODIUM TO PREVENT SUDDEN INCREASE IN THE LEVELS OF LITHIUM LEADING TO TOXICITY AND DEATH.
40. THE CLIENT HAS BEEN TAKING CLOMIPRAMINE (ANAFRANIL) FOR HIS OBSESSIVE-COMPULSIVE DISORDER. HE TELLS THE NURSE, "I'M NOT REALLY BETTER, AND I'VE BEEN TAKING THE MEDICATION FAITHFULLY FOR THE PAST 3 DAYS JUST LIKE IT SAYS ON THIS PRESCRIPTION BOTTLE." WHICH OF THE FOLLOWING ACTIONS WOULD THE NURSE DO FIRST?
A. TELL THE CLIENT TO CONTINUE TAKING THE MEDICATION AS PRESCRIBED BECAUSE IT TAKES 5 TO 10 WEEKS FOR A FULL THERAPEUTIC EFFECT. : ANAFRANIL IS AN ANTI DEPRESSANT, EFFECTS ARE NOTICEABLE WITHIN 1 TO 2 WEEKS.
41. THE NURSE JUDGES CORRECTLY THAT A CLIENT IS EXPERIENCING AN ADVERSE EFFECT FROM AMITRIPTYLINE HYDROCHLORIDE (ELAVIL) WHEN THE CLIENT DEMONSTRATES:
D. URINARY RETENTION : ELAVIL IS AN TC ANTIDEPRESSANT. IT SHOULD NOT CAUSE INSOMNIA. HYPERTENSION ARE SPECIFIC OF MAOI ANTI DEPRESSANTS WHEN TYRAMINE IS INGESTED. DUE TO THE ANTICHOLINERGIC S/E OF TCAS, URINARY RETENTION IS AN ADVERSE EFFECT.
42. WHICH OF THE FOLLOWING HEALTH STATUS ASSESSMENTS MUST BE COMPLETED BEFORE THE CLIENT STARTS TAKING IMIPRAMINE (TOFRANIL)?
A. ELECTROCARDIOGRAM (ECG). : ASIDE FROM TONOMETRY OR IOP MEASUREMENT, CLIENT SHOULD UNDERGO REGULAR ECG SCHEDULE. MOST TCAS CAUSSE TACHYCARDIAS AND ECG CHANGES, AN ECG SHOULD BE DONE BEFORE THE CLIENT TAKES THE MEDICATION.
43. A CLIENT COMES TO THE OUTPATIENT MENTAL HEALTH CLINIC 2 DAYS AFTER BEING DISCHARGED FROM THE HOSPITAL. THE CLIENT WAS GIVEN A 1-WEEK SUPPLY OF CLOZAPINE (CLOZARIL). THE NURSE REVIEWS INFORMATION ABOUT CLOZAPINE WITH THE CLIENT. WHICH CLIENT STATEMENT INDICATES AN ACCURATE UNDERSTANDING OF THE NURSE'S TEACHING ABOUT THIS MEDICATION?
B."I NEED TO KEEP MY APPOINTMENT HERE AT THE HOSPITAL THIS WEEK FOR A BLOOD TEST." : REGULAR BLOOD CHECK UP IS REQUIRED FOR PATIENTS TAKING CLOZARIL. AS FREQUENT AS EVERY 2 WEEKS. CLOZAPINE CAN CAUSE BONE MARROW DEPRESSION, THEREFORE, FREQUENT BLOOD COUNTS ARE NECESSARY.
44. THE CLIENT IS TAKING RISPERIDONE (RISPERDAL) TO TREAT THE POSITIVE AND NEGATIVE SYMPTOMS OF SCHIZOPHRENIA. WHICH OF THE FOLLOWING NEGATIVE SYMPTOMS WILL IMPROVE?.
D. ASOCIAL BEHAVIOUR AND ANERGIA : A,B AND C ARE ALL POSITIVE SYMPTOMS OF SCHIZOPHRENIA. NEGATIVE SYMPTOMS INCLUDES ANHEDONIA, ANERGIA, ASSOCIATIVE LOOSENESS AND ASOCIAL BEHAVIOR.
45. THE NURSE WOULD TEACH THE CLIENT TAKING TRANYLCYPROMINE SULFATE (PARNATE) TO AVOID WHICH FOOD BECAUSE OF ITS HIGH TYRAMINE CONTENT?
B. AGED CHEESES. : THIS IS HIGH IN TYRAMINE, AND THEREFORE, REMOVED FROM PATIENTS DIET TO PREVENT HYPERTENSIVE CRISIS.
46. WHICH OF THE FOLLOWING CLINICAL MANIFESTATIONS WOULD ALERT THE NURSE TO LITHIUM TOXICITY?
D.ANOREXIA WITH NAUSEA AND VOMITING.
47. THE CLIENT WITH DEPRESSION HAS BEEN HOSPITALIZED FOR 3 DAYS ON THE PSYCHIATRIC UNIT. THIS IS THE SECOND HOSPITALIZATION DURING THE PAST YEAR. THE PHYSICIAN ORDERS A DIFFERENT DRUG, TRANYLCYPROMINE SULFATE (PARNATE), WHEN THE CLIENT DOES NOT RESPOND POSITIVELY TO A TRICYCLIC ANTIDEPRESSANT. WHICH OF THE FOLLOWING REACTIONS SHOULD THE CLIENT BE CAUTIONED ABOUT IF HER DIET INCLUDES FOODS CONTAINING TRYAMINETYRAMINE?
D. HYPERTENSIVE CRISIS.
48. AFTER THE NURSE HAS TAUGHT THE CLIENT WHO IS BEING DISCHARGED ON LITHIUM (ESKALITH) ABOUT THE DRUG, WHICH OF THE FOLLOWING CLIENT STATEMENTS WOULD INDICATE THAT THE TEACHING HAS BEEN SUCCESSFUL?
C. "I'LL CALL MY DOCTOR RIGHT AWAY FOR ANY VOMITING, SEVERE HAND TREMORS, OR MUSCLE WEAKNESS." : THIS IS A SIGN OF LIGHT LITHIUM TOXICITY. INCREASING FLUID INTAKE WILL CAUSE DILUTIONAL DECREASE OF LITHIUM LEVEL. RESTRICTION OF SODIUM WILL CAUSE DILUTIONAL INCREASE IN LITHIUM LEVEL.
49. A NURSE IS CARING FOR A CLIENT WITH PARKINSON'S DISEASE WHO HAS BEEN TAKING CARBIDOPA/LEVODOPA (SINEMET) FOR A YEAR. WHICH OF THE FOLLOWING ADVERSE REACTIONS WILL THE NURSE MONITOR THE CLIENT FOR?
C. HYPOTENSION : HYPOTENSION, DIZZINESS AND LETHARGY ARE SIDE EFFECTS OF ANTI PARKINSON DRUGS LIKE LEVODOPA AND CARBIDOPA.
50. A CLIENT IS TAKING FLUOXETINE HYDROCHLORIDE (PROZAC) FOR TREATMENT OF DEPRESSION. THE CLIENT ASKS THE NURSE WHEN THE MAXIMUM THERAPEUTIC RESPONSE OCCURS. THE NURSE'S BEST RESPONSE IS THAT THE MAXIMUM THERAPEUTIC RESPONSE FOR FLUOXETINE HYDROCHLORIDE MAY OCCUR IN THE:
C. THIRD WEEK : A AND B ARE SIMILAR, THEREFORE , REMOVED THEM FIRST. RECOGNIZING THAT MOST ANTIDEPRESSANTS EXERTS THEIR EFFECTS WITHIN 2-3 WEEKS WILL LEAD YOU TO LETTER C.
OB QUESTIONS I
1. I n the 12th week gestation a client completely expels the products of conception. Because the client is Rh negative, the nurse must:
a. Administer RhoGAM within 72 hours
b. Make certain she receives RhoGAM on her first clinic visit
c. Not give RhoGAM, since it is not used with the birth of a stillborn
d. Make certain the client does not receive RhoGAM, since the gestation was 12 weeks
2. A pregnant client develops thrombophlebitis of the left leg and admitted to the hospital for bed rest and anticoagulant therapy. The anticoagulant the nurse should expect to administer is:
a. Heparin
b. Dicumarol
c. Diphenadione (Dipaxin)
d. Warfarin
3. A client, undergoing treatment for infertility, is diagnosed as having endometriosis. The nurse is aware that one of the drugs that may used to treat this condition is:
a. Relaxin (Releasin)
b. Leuprolide (lupron)
c. Ergonovine (Ergotrate)
d. Esterified estrogen (Climestrone)
4. During labor a client who has been receiving epidural anesthesia has a sudden episode of severe nausea, and her skin becomes pale and clammy. The nurse’s immediate reaction is to:
a. Notify the physician
b. Elevate the client’s legs
c. Check for vaginal bleeding
d. Monitor for FHR every 3 minutes
5. A client at 6 weeks gestation is receiving antibiotics therapy for pyelonephritis. The nurse is aware that the safest antibiotic for administration during pregnancy is:
a. Gastrisin
b. Ampicillin
c. Tetracycline
d. Nitrofurantoin
6. A client who was admitted in active labor has only progressed from 2 cm to 3 cm in 8 hours. She is diagnosed as having hypotic dystocia and is given oxytocin (Pitocin) to augment her contraction. The most important aspect of nursing at this time is:
a. Monotoring the FHR
b. Checking perineum for bulging
c. Timing and recording length of contraction
d. Preparing for emergency cesarean delivery
7. A client, 38 weeks gestation, is admitted for induction of labor. She has history of ruptured membranes for the past 12 hours. She has no other symptoms of labor. The nurse is aware that if the proper conditons exist, the physician will prescribe:
a. Progesterone
b. Oxytocin (Pitocin)
c. Lututrin (Lutraxin)
d. Ergonovine maleate
8. At about 5 cm, a laboring client receives medication for pain. The nurse is aware that one of the medications given to women in labor that could cause respiratory depression of newborn is:
a. Scopolamine
b. Promazine (Sparine)
c. Meperidine (Demerol)
d. Promethazine (Phenegran)
9. A client is the midphase of labor becomes very uncomfortable and asks for medication. Meperidine (Demerol) 50 mg and phenergan 50 mg are ordered. These medications:
a. Act to produce amnesia
b. Act as preliminary anesthestics
c. Induce the sleep until the time of delivery
d. Increase the client’s pain threshold, resulting in relaxation
10. A client begins preterm labor and the physician orders terbutaline sulfate ( Brethine). After its administration, the nurse assesses the client for the therapeutic effect of:
a. Reduction of pain in the perineal area
b. Decrease in blood pressure from 120/80 to 90/60
c. Decrease in frequency and duration of contractions
d. Dilation of the cervix from 1 to 1.5 cm for every hour of labor
11. A client is on magnesium sulfate therapy for severe preeclampsia. The nurse must be alert for the first sign of an excessive blood magnesium level, which is:
a. Disturbance in sensorium
b. Increase in respiratory rate
c. Development of cardiac dysrhythmia
d. Disappearance of the knee-jerk reflex
12. The following delivry a cardiac client with type 2 diabetes asks the nurse, “ Which contraceptives will I be able to use to prevent pregnancy in the near future? The nurse’s best response would be:
a. “You may use oral contraceptives. They are almost 100% effective in preventing pregnancy
b. “ You may want to use foam and a condom to prevent pregnancy until you consult with your doctor at your postpartum visit.”
c. “ The intrauterine device is best for you because it does not allow a fertilizes ovum to become implanted into the uterine lining
d. “You do not need to worry about becoming pregnant in the near future. Clients with cardiac conditions usually become fertile
13. The nurse teaches that the most frequent side effect associated with the use of IUDs is:
a. Ectopic pregnancy
b. Expulsion of the IUD
c. Rupture of the uterus
d. Excessive menstrual flow
14. The nurse should explain that the common problem that has been associates with IUDs when they are used, is:
a. Perforation of the uterus
b. Discomfort associated with coitus
c. Development of vaginal infection
d. Spontaneous expulsion of the device
15. A client seeking advice about contraception asks the nurse about an IUD. The nurse explains that the IUD provides contraception by:
a. Blocking the cervical os
b. Increasing the mobility of the uterus
c. Preventing the sperm from reaching the fallopian tube
d. Setting up a nonspecific inflammatory cell reaction in the endometrium
16. In a lecture on sexual functioning, the nurse plans to include the fact that ovulation occurs when the:
a. Oxytocin level is high
b. Blood level of LH is high
c. Progesterone level is high
d. Endometrial wall is sloughed off
17. After ovulation has occurred, the ovum is believed to remain viable for:
a. 1 to 6 hours
b. 12 to 18 hours
c. 24 to 36 hours
d. 48 to 72 hours
18. The time of ovulation can be determined by taking the basal temperature. During ovulation the basal temperature:
a. Drops markedly
b. Drops slightly and then rises
c. Rises suddenly and the falls
d. Rises markedly and remains high
19. When an oral contraceptives are prescribed for a client the nurse should teach the client about potential of developing:
a. Cervicitis
b. Ovarian cysts
c. Rises suddenly and then falls
d. Rises marked and remains high
20. The nurse explains that the efficiencyof the basla body temperature (BBT) method of contraception depends on the fluctuation of the basal body temperature. A factor that will alter its effectiveness is:
a. Presence of stress
b. Length of abstinence
c. Age of those involved
d. Frequency of intercourse
21. A biphasic antiovulatory medication of combined progestin and estrogen is prescribed for female client. The nurse, instructing the client about the medication, should include the need to:
a. Edema
b. Oliguria
c. Headache
d. Bradycardia
22. The following a salinization procedure for elective abortion of a 20-week pregnancy, the client is told that labor will probably begin within:
a. Two hours after the procedure
b. Four hours following the procedure
c. Eight to 24 hous after the procedure
d. Several minutes following the procedure
23. In the dilation and suction evacuation method of elective abortion, Laminaria is used in dilation stage of procedure because:
a. Dilation occurs within 2 hours
b. They are hygroscopic and expand
c. They are stronger in action than instruments
d. Less anesthesia is necessary with this method.
Communicable Disease Nursing
DRUG OF CHOICE
Tetanus: PEN G Na; DIAZEPAM (Valium)
Meningitis: MANNITOL (osmotic diuretic); DEXAMETHASONE (anti-inflammatory); DILANTIN/PHENYTOIN (anti-convulsive); PYRETINOL/ENCEPHABO L (CNS stimulant)
Rabies Vaccines: LYSSAVAC, VERORAB
Immunoglobulins: ERIG or HRIg
DIAGNOSTIC TESTS
Tetanus: WOUND CULTURE
Meningitis: LUMBAR PUNCTURE
Encephalitis: EEG
Polio: EMG; Muscle testing
Rabies: Brain biopsy (Negri bodies) Fluorescent rabies antibody test
Dengue: TOURNIQUET test (Rumpel lead)
Malaria: Malarial smear; QBC (Quantitative Buffy Coat)
Scarlet: DICK'S TEST; SCHULTZ-CHARLTON TEST
Diphtheria: SCHICK'S TEST; Moloney's Test
Pertussis: Nasal swab; agar plate
Tuberculosis: MANTOUX test
Leprosy: SLIT SKIN SMEAR
Pinworm: SCOTCH TAPE SWAB
Typhoid: WIDAL'S test
HIV/AIDS: ELISA; WESTERN BLOT; PCT: Polymerase Chain Reaction Test
CAUSATIVE AGENTS
Tetanus: CLOSTRIDIUM TETANI
Meningococcemia: NEISSERIA MENINGITIDIS
Rabies: RHABDOVIRUS
Poliomyelitis: LEGIO DEBILITANS (Type I Brunhilde); (Type II Lansing); (Type III Leon)
Dengue Fever: ARBOVIRUSES (Chikunggunya); (Onyong-nyong); (West Nile); (Flaviviruses) (Common in the Phil.)
Malaria: PLASMODIUM (protozoa) P. Falciparum (most fatal); P. Vivax P. Malariae; P. Ovale
Filariasis: WUCHERERIA BANCROFTI; BRUGIA MALAYI
Leprosy: MYCOBACTERIUM LEPRAE
Measles: PARAMYXO VIRUS
German measles: TOGA VIRUS
Chicken pox: VARICELLA ZOSTER VIRUS
Herpes zoster: HERPES ZOSTER VIRUS
Scarlet fever: Group A HEMOLYTIC STREPTOCOCCUS
Scabies: SARCOPTES SCABIEI (itch mite)
Bubonic plague: YERSINIA PESTIS
Diphtheria: KLEBS LOEFFLER
Pertussis: BORDETELLA PERTUSSIS
Tuberculosis: MYCOBACTERIUM TUBERCULOSIS
Typhoid: SALMONELLA TYPHI
Cholera: VIBRIO CHOLERA
Amoebiasis: ENTAMOEBA HYSTOLITICA
Leptospirosis: LEPTOSPIRA Spirochete
Schistosomiasis: Schistosoma japonicum
Gonorrhea: N. GONORRHEAE
Syphilis: TREPONEMA PALLIDUM
Chlamydia: C. trachomatis, T. vaginalis
Genital herpes: HERPES SIMPLEX 2
CD PHARMACOLOGY
Malaria: CHLOROQUINE
Schistosomiasis: PRAZIQUANTEL
Scabies: EURAX/ CROTAMITON
Chicken pox: ACYCLOVIR/ZOVIRAX
Tuberculosis: R.I.P.E.S.
Pneumonia: COTRIMOXAZOLE; Procaine Penicillin
Helminths: MEBENDAZOLE; PYRANTEL PAMOATE
Newborn Screening
Newborn Screening (NBS) is a simple procedure to find out if your baby has a congenital metabolic disorder that may lead to mental retardation and even death if left untreated.
Why is it important to have Newborn Screening?
Most babies with metabolic disorders look normal at birth. One will never know that the baby has the disorder until the onset of signs and symptoms and more often ill effects are already irreversible.
When is Newborn Screening done?
Newborn screening is ideally done on the 48th hour or at least 24 hours from birth. Some disorders are not detected if the test is done earlier than 24 hours. The baby must be screened again after 2 weeks for more accurate results.
How is Newborn Screening done?
Newborn screening is a simple procedure. Using the heel prick method, a few drops are taken from the baby's heel and blotted on a special absorbent filter card. The blood is dried for 4 hours and sent to the Newborn Screening Laboratory. (NBS Lab).
Who will collect the sample for Newborn Screening?
A physician, a nurse, a midwife or medical technologist can do the newborn screening.
Where is Newborn Screening Available?
Newborn screening is available in practicing health institutions (hospitals, lying-ins, Rural Health Units and Health Centers). If babies are delivered at home, babies may be brought to the nearest institution offering newborn screening.
When is the Newborn Screening results available?
Newborn screening results are available within three weeks after the NBS Lab receives and tests the samples sent by the institutions. Results are released by NBS Lab to the institutions and are released to your attending birth attendants or physicians. Parents may seek the results from the institutions where samples are collected.
A negative screen mean that the result of the test is normal and the baby is not suffering from any of the disorders being screened.
In case of a positive screen, the NBS nurse coordinator will immediately inform the coordinator of the institution where the sample was collected for recall of patients for confirmatory testing.
What should be done when a baby has a positive newborn screening result?
Babies with positive results should be referred at once to the nearest hospital or specialist for confirmatory test and further management. Should there be no specialist in the area, the NBS secretariat office will assist its attending physician.
Source: doh.gov.ph
Note: This was a community health nursing board question last June. The one that I italicized were the answers to the questions asked. So I advice you guys especially those taking the December exam to be abreast with the new laws affecting the practice of nursing profession in the Philippines.
INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS
THE INEQUITIES OF CHILD HEALTH
Although the annual number of deaths among children less than 5 years old has decreased by almost a third since the 1970s,
this reduction has not been evenly distributed throughout the world. According to the 1999 World Health Report, children
in low- to
middle-income countries are 10 times more likely to die before reaching age 5 than children living in the industrialised world.
In 1998, more than 50 countries still had childhood mortality rates of over 100 per 1,000 live births.
Every year more than 10 million children in these countries die before they reach their fifth birthday.
Seven in 10 of these deaths are due to acute respiratory infections (mostly pneumonia), diarrhoea, measles, malaria, o
r malnutrition — and often to a combination of these conditions.
Distribution of 10.5 Million Deaths Among Children Less Than 5 Years Old in All Developing Countries, 1999
Projections based on the 1996 analysis The Global Burden of Disease indicate that these conditions will continue to be major
contributors to child deaths through the year 2020 unless significantly greater efforts are made to control them.
Infant and childhood mortality are sensitive indicators of inequity and poverty.
It is no surprise to find that the children who are most commonly and severely ill, who are malnourished and who are most
likely to die of their illness are
those of the most vulnerable and underprivileged populations of low-income countries. However, even within middle-income a
nd so-called industrialised countries, there are often neglected geographical areas where childhood mortality remains high.
Millions of children in these areas are often caught in the vicious cycle of poverty and ill health — poverty leads to ill
health and ill health breeds poverty.
Quality of care is another important indicator of inequities in child health.
Every day, millions of parents seek health care for their sick children, taking them to hospitals, health centres, pharmacists,
doctors, and traditional healers. Surveys reveal that many sick children are not properly assessed and treated by these health
providers, and that their parents are poorly advised. At first-level health facilities in low-income countries, diagnostic
supports
such as radiology and laboratory services are minimal or non-existent, and drugs and equipment are often scarce.
Limited supplies
and equipment, combined with an irregular flow of patients, leave doctors at this level with few opportunities to practise
complicated clinical procedures. Instead, they often rely on history and signs and symptoms to determine a course of management
that makes the best use of available resources.
Providing quality care to sick children in these conditions is a serious challenge. Yet how can this situation be reversed?
Experience and scientific evidence show that improvements in child health are not necessarily dependent on the use of sophisticated
and expensive technologies, but rather on effective strategies that are based on a holistic approach, are available to the majority
of those in need, and which take into account the capacity and structure of health systems, as well as traditions and
beliefs in the
community.
RATIONALE FOR AN EVIDENCE-BASED SYNDROMIC APPROACH TO CASE MANAGEMENT
Many well-known prevention and treatment strategies have already proven effective for saving young lives.
Childhood vaccinations have successfully reduced deaths due to measles. Oral rehydration therapy has contributed to a
major reduction in diarrhoea deaths.
Effective antibiotics have saved millions of children with pneumonia. Prompt treatment of malaria has allowed more
children to recover and lead healthy lives. Even modest improvements in breastfeeding practices have reduced childhood deaths.
While each of these interventions has shown great success, accumulating evidence suggests that a more integrated approach to
managing sick children is needed to achieve better outcomes.
Child health programmes need to move beyond single diseases to
addressing the overall health and well-being of the child. Because many children present with overlapping signs and symptoms
of diseases, a single diagnosis can be difficult, and may not be feasible or appropriate. This is especially true for
first-level health facilities where examinations involve few instruments, little or no laboratory tests, and no X-ray.
During the mid-1990s, the World Health Organization (WHO), in collaboration with UNICEF and many other agencies, institutions
and individuals, responded to this challenge by developing a strategy known as the Integrated Management of Childhood
Illness (IMCI).
Although the major reason for developing the IMCI strategy stemmed from the needs of curative care, the strategy also
addresses aspects of nutrition, immunization, and other important elements of disease prevention and health promotion
. The objectives of the strategy are to reduce death and the frequency and severity of illness and disability, and to
contribute to improved growth and development.
The IMCI clinical guidelines target children less than 5 years old — the age group that bears the highest burden of
deaths from common
childhood diseases
Proportion of Global Burden of Selected Diseases Borne by Children Under 5 Years (Estimated, Year 2000)
The guidelines take an evidence-based, syndromic approach to case management that supports the rational, effective a
nd affordable use of drugs and diagnostic tools. Evidence-based medicine stresses the importance of evaluation of ev
idence from clinical research and cautions against the use of intuition, unsystematic clinical experience, and untes
ted pathophysiologic reasoning for medical decision-making. In situations where laboratory support and clinical res
ources are limited, the syndromic approach is a more realistic and cost-effective way to manage patients. Careful an
d systematic assessment of common symptoms and well-selected clinical signs provides sufficient information to guide
rational and effective actions.
An evidence-based syndromic approach can be used to determine the:
• Health problem(s) the child may have;
• Severity of the child’s condition;
• Actions that can be taken to care for the child (e.g. refer the child immediately, manage with available
resources, or manage at home).
In addition, IMCI promotes:
• Adjustment of interventions to the capacity and functions of the health system; and
• Active involvement of family members and the community in the health care process.
Parents, if correctly informed and counselled, can play an important role in improving the health status of
their children by following the advice given by a health care provider, by applying appropriate feeding practi
ces and by bringing sick children to a health facility as soon as symptoms arise. A critical example of the need
for timely care is Africa, where approximately 80 percent of childhood deaths occur at home, before the child has
any contact with a health facility.
COMPONENTS OF THE INTEGRATED APPROACH
The IMCI strategy includes both preventive and curative interventions that aim to improve practices in health
facilities, the health system and at home. At the core of the strategy is integrated case management of the most c
ommon childhood problems with a focus on the most common causes of death.
The strategy includes three main components:
• Improvements in the case-management skills of health staff through the provision of locally-adapted
guidelines on integrated management of childhood illness and activities to promote their use;
• Improvements in the overall health system required for effective management of childhood illness;
• Improvements in family and community health care practices.
THE PRINCIPLES OF INTEGRATED CARE
The IMCI guidelines are based on the following principles:
• All sick children must be examined for “general danger signs” which indicate the need for
immediate referral or admission to a hospital.
• All sick children must be routinely assessed for major symptoms (for children age 2 months up to 5
years: cough or difficult breathing, diarrhoea, fever, ear problems; for young infants age 1 week up to 2
months: bacterial infection and diarrhoea). They must also be routinely assessed for nutritional and immunization
status, feeding problems, and other potential problems.
• Only a limited number of carefully-selected clinical signs are used, based on evidence of their
sensitivity and specificity to detect disease. These signs were selected considering the conditions and
realities of first-level health facilities.
• A combination of individual signs leads to a child’s classification(s) rather than a diagnosis.
Classification(s) indicate the severity of condition(s). They call for specific actions based on whether
the child (a) should be urgently referred to another level of care, (b) requires specific treatments
(such as antibiotics or antimalarial treatment), or (c) may be safely managed at home. The
classifications are colour coded: “pink” suggests hospital referral or admission, “yellow” indicates
initiation of treatment, and “green” calls for home treatment.
• The IMCI guidelines address most, but not all, of the major reasons a sick child is brought to a clinic.
A child returning with chronic problems or less common illnesses may require special care. The guidelines do not
describe the management of trauma or other acute emergencies due to accidents or injuries.
• IMCI management procedures use a limited number of essential drugs and encourage active participation
of caretakers in the treatment of children.
• An essential component of the IMCI guidelines is the counselling of caretakers about home care,
including counselling about feeding, fluids and when to return to a health facility.
ADAPTING THE GUIDELINES TO A COUNTRY’S SITUATION
The underlying principles of the IMCI guidelines are constant. However, in each country the IMCI clinical
guidelines should be adapted to:
• Cover the most serious childhood illnesses typically seen at first-level health facilities;
• Make the guidelines consistent with national treatment guidelines and other policies; and
• Make IMCI implementation feasible through the health system and by families caring for their children at home.
Adaptation of the IMCI guidelines normally is co-ordinated by a national health regulating body
(e.g., Ministry of Health) and incorporates decisions carefully made by national health experts.
For this reason, some clinical signs and details of clinical procedures described below may differ
from those used in a particular country. The principles used for management of sick children, however,
are fully applicable in all situations.
THE IMCI CASE MANAGEMENT PROCESS
The case management of a sick child brought to a first-level health facility includes a number of important
elements (see Figure 3).
Outpatient Health Facility
• Assessment;
• Classification and identification of treatment;
• Referral, treatment or counselling of the child’s caretaker (depending on the classification(s) identified);
• Follow-up care.
Referral Health Facility
• Emergency triage assessment and treatment (ETAT);
• Diagnosis, treatment and monitoring of patient progress.
Appropriate Home Management
• Teaching mothers or other caretakers how to give oral drugs and treat local infections at home;
• Counselling mothers or other caretakers about food (feeding recommendations, feeding problems);
fluids; when to return to the health facility; and her own health.
Depending on a child’s age, various clinical signs and symptoms have different degrees of reliability
and diagnostic value and importance. Therefore, the IMCI guidelines recommend case management
procedures based on two age categories:
• Children age 2 months up to 5 years
• Young infants age 1 week up to 2 months
IMCI Case Management in the Outpatient Health Facility,
First-level Referral Facility and at Home
For the Sick Child From Age 2 Months up to 5 Years
OUTPATIENT MANAGEMENT OF CHILDREN
AGE 2 MONTHS UP TO 5 YEARS
ASSESSMENT OF SICK CHILDREN
The assessment procedure for this age group includes a number of important steps that must be taken
by the health care provider, including: (1) history taking and communicating with the caretaker
about the child’s problem; (2) checking for general danger signs; (3) checking main symptoms; (4)
checking nutritional status; (5) assessing the child’s feeding; (6) checking immunization status;
and (7) assessing other problems.
COMMUNICATING WITH THE CARETAKER
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
It is critical to communicate effectively with the child's mother or caretaker. Good communication
techniques and an integrated assessment are required to ensure that common problems or signs of
disease or malnutrition are not overlooked. Using good communication helps to reassure the mother
or caretaker that the child will receive good care. In addition, the success of home treatment
depends on how well the mother or caretaker knows how to give the treatment and understands its importance.
The steps to good communication are:
• Listen carefully to what the caretaker says. This will show them that you take their concerns seriously.
• Use words the caretaker understands. Try to use local words and avoid medical terminology.
• Give the caretaker time to answer questions. S/he may need time to reflect and decide if a clinical sign is present.
• Ask additional questions when the caretaker is not sure about the answer. A caretaker may not
be sure if a symptom or clinical sign is present. Ask additional questions to help her/him give clear answers.
CHECKING FOR GENERAL DANGER SIGNS
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
A sick child brought to an outpatient facility may have signs that clearly indicate a specific problem.
For example, a child may present with chest indrawing and cyanosis, which indicate severe pneumonia.
However, some children may present with serious, non-specific signs called "general danger signs" that
do not point to a particular diagnosis. For example, a child who is lethargic or unconscious may have
meningitis, severe pneumonia, cerebral malaria or another severe disease. Great care should be taken to
ensure that these general danger signs are not overlooked because they suggest that a child is severely
ill and needs urgent attention.
The following danger signs should be routinely checked in all children.
• The child has had convulsions during the present illness. Convulsions may be the result of fever.
In this instance, they do little harm beyond frightening the mother. On the other hand, convulsions may be
associated with meningitis, cerebral malaria or other life threatening conditions. All children who have had
convulsions during the present illness should be considered seriously ill.
• The child is unconscious or lethargic. An unconscious child is likely to be seriously ill. A
lethargic child, who is awake but does not take any notice of his or her surroundings or does not
respond normally to sounds or movement, may also be very sick. These signs may be associated with many conditions.
• The child is unable to drink or breastfeed. A child may be unable to drink either because s/he is
too weak or because s/he cannot swallow. Do not rely completely on the mother's evidence for this,
but observe while she tries to breastfeed or to give the child something to drink.
• The child vomits everything. The vomiting itself may be a sign of serious illness, but it is also
important to note because such a child will not be able to take medication or fluids for rehydration.
If a child has one or more of these signs, s/he must be considered seriously ill and will almost always
need referral. In order to start treatment for severe illnesses without delay, the child should be quickly
assessed for the most important causes of serious illness and death — acute respiratory infection (ARI),
diarrhoea, and fever (especially associated with malaria and measles). A rapid assessment of nutritional
status is also essential, as malnutrition is another main cause of death.
CHECKING MAIN SYMPTOMS
After checking for general danger signs, the health care provider must check for main symptoms. The
generic IMCI clinical guidelines suggest the following four: (1) cough or difficult breathing; (2)
diarrhoea; (3) fever; and (4) ear problems.
The first three symptoms are included because they often result in death. Ear problems are included
because they are considered one of the main causes of childhood disability in low- and middle-income countries.
COUGH OR DIFFICULT BREATHING
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
A child presenting with cough or difficult breathing should first be assessed for general danger signs.
This child may have pneumonia or another severe respiratory infection. After checking for danger signs,
it is essential to ask the child’s caretaker about this main symptom.
Clinical Assessment
Three key clinical signs are used to assess a sick child with cough or difficult breathing:
• Respiratory rate, which distinguishes children who have pneumonia from those who do not;
• Lower chest wall indrawing, which indicates severe pneumonia; and
• Stridor, which indicates those with severe pneumonia who require hospital admission.
No single clinical sign has a better combination of sensitivity and specificity to detect pneumonia in children
under 5 than respiratory rate, specifically fast breathing. Even auscultation by an expert is less sensitive as a single sign.
Cut-off rates for fast breathing (the point at which fast breathing is considered to be fast) depend on the
child’s age. Normal breathing rates are higher in children age 2 months up to 12 months than in children age
12 months up to 5 years.
Child’s Age Cut-off Rate for Fast Breathing
2 months up to 12 months 50 breaths per minute or more
12 months up to 5 years 40 breaths per minute or more
Note: The specificity of respiratory rate for detecting pneumonia depends on the prevalence of bacterial
pneumonia among the population. In areas with high levels of viral pneumonia, respiratory rate has
relatively modest specificity. Nevertheless, even if the use of respiratory rate leads to some overtreatment,
this will still be small compared with the current use of antibiotics for all children with an ARI, as occurs in many clinics.
Lower chest wall indrawing, defined as the inward movement of the bony structure of the chest wall with
inspiration, is a useful indicator of severe pneumonia. It is more specific than “intercostal indrawing,”
which concerns the soft tissue between the ribs without involvement of the bony structure of the chest wall.
Chest indrawing should only be considered present if it is consistently present in a calm child. Agitation, a
blocked nose or breastfeeding can all cause temporary chest indrawing.
Stridor is a harsh noise made when the child inhales (breathes in). Children who have stridor when calm have a
substantial risk of obstruction and should be referred. Some children with mild croup have stridor only when
crying or agitated. This should not be the basis for indiscriminate referral. Sometimes a wheezing noise is
heard when the child exhales (breathes out). This is not stridor. A wheezing sound is most often associated
with asthma. Experience suggests that even where asthma rates are high, mortality from asthma is relatively
uncommon. In some cases, especially when a child has wheezing when exhaling, the final decision on presence
or absence of fast breathing can be made after a test with a rapid acting bronchodilator (if available). At
this level, no distinction is made between children with bronchiolitis and those with pneumonia.
Classification of Cough or Difficult Breathing
Based on a combination of the above clinical signs, children presenting with cough or difficult breathing can be
classified into three categories:
• Those who require referral for possible SEVERE PNEUMONIA OR VERY SEVERE DISEASE.
This group includes children with any general danger sign, or lower chest indrawing or stridor when calm. Children with
SEVERE PNEUMONIA OR VERY SEVERE DISEASE most likely will have invasive bacterial organisms and diseases that may be
life-threatening. This warrants the use of injectable antibiotics.
• Those who require antibiotics as outpatients because they are highly likely to have bacterial PNEUMONIA.
This group includes all children with fast respiratory rate for age. Fast breathing, as defined by WHO, detects about 80
percent of children with pneumonia who need antibiotic treatment. Treatment based on this classification has been shown
to reduce mortality.
• Those who simply have a COUGH OR COLD and do not require antibiotics.
Such children may require a safe remedy to a relieve cough. A child with cough and cold normally improves in one or
two weeks. However, a child with chronic cough (more than 30 days) needs to be further assessed (and, if needed, referred)
to exclude tuberculosis, asthma, whooping cough or another problem.
DIARRHOEA
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
A child presenting with diarrhoea should first be assessed for general danger signs and the child's caretaker should be
asked if the child has cough or difficult breathing.
Diarrhoea is the next symptom that should be routinely checked in every child brought to the clinic. A child with
diarrhoea may have three potentially lethal conditions: (1) acute watery diarrhoea (including cholera); (2) dysentery
(bloody diarrhoea); and (3) persistent diarrhoea (diarrhoea that lasts more than 14 days). All children with diarrhoea
should be assessed for: (a) signs of dehydration; (b) how long the child has had diarrhoea; and (c) blood in the stool
to determine if the child has dysentery.
Clinical Assessment
All children with diarrhoea should be checked to determine the duration of diarrhoea, if blood is present in the
stool and if dehydration is present. A number of clinical signs are used to determine the level of dehydration:
Child’s general condition. Depending on the degree of dehydration, a child with diarrhoea may be lethargic or
unconscious (this is also a general danger sign) or look restless/irritable. Only children who cannot be
consoled and calmed should be considered restless or irritable.
Sunken eyes. The eyes of a dehydrated child may look sunken. In a severely malnourished child who is visibly
wasted (that is, who has marasmus), the eyes may always look sunken, even if the child is not dehydrated.
Even though the sign “sunken eyes” is less reliable in a visibly wasted child, it can still be used to
classify the child's dehydration.
Child’s reaction when offered to drink. A child is not able to drink if s/he is not able to take fluid in his/her mouth and
swallow it. For example, a child may not be able to drink because s/he is lethargic or unconscious. A child is drinking
poorly if the child is weak and cannot drink without help. S/he may be able to swallow only if fluid is put in his/her mouth.
A child has the sign drinking eagerly, thirsty if it is clear that the child wants to drink. Notice if the child reaches
out for the cup or spoon when you offer him/her water. When the water is taken away, see if the child is unhappy because
s/he wants to drink more. If the child takes a drink only with encouragement and does not want to drink more, s/he does
not have the sign “drinking eagerly, thirsty.”
Elasticity of skin. Check elasticity of skin using the skin pinch test. When released, the skin pinch goes back either very
slowly (longer than 2 seconds), or slowly (skin stays up even for a brief instant), or immediately. In a child with marasmus
(severe malnutrition), the skin may go back slowly even if the child is not dehydrated. In an overweight child, or a child with
oedema, the skin may go back immediately even if the child is dehydrated.
After the child is assessed for dehydration, the caretaker of a child with diarrhoea should be asked how long the child has had
diarrhoea and if there is blood in the stool. This will allow identification of children with persistent diarrhoea and dysentery.
Classification of Dehydration
Based on a combination of the above clinical signs, children presenting with diarrhoea are classified into three categories:
• Those who have SEVERE DEHYDRATION and who require immediate IV infusion, nasogastric or oral fluid replacement
according to the WHO treatment guidelines described in Plan C (see figure 4 under treatment procedures).
Patients have severe dehydration if they have a fluid deficit equalling greater than 10 percent of their body weight. A child is
severely dehydrated if he/she has any combination of two of the following signs: is lethargic or unconscious, is not able to drink
or is drinking poorly, has sunken eyes, or a skin pinch goes back very slowly.
• Those who have SOME DEHYDRATION and who require active oral treatment with ORS solution according to WHO treatment
guidelines described in Plan B (see figure 5 under treatment procedures).
Children who have any combination of the following two signs are included in this group:
restless/irritable, sunken eyes, drinks eagerly/thirsty, skin pinch goes back slowly. Children with some dehydration have a fluid
deficit equalling 5 to 10 percent of their body weight. This classification includes both "mild" and "moderate” dehydration,
which are descriptive terms used in most paediatric textbooks.
• Those children with diarrhoea who have NO DEHYDRATION.
Patients with diarrhoea but no signs of dehydration usually have a fluid deficit, but equal to less than 5 percent of their
body weight. Although these children lack distinct signs of dehydration, they should be given more fluid than usual to prevent
dehydration from developing as specified in WHO Treatment Plan A (see figure 5 under treatment procedures).
Note: Antibiotics should not be used routinely for treatment of diarrhoea. Most diarrhoeal episodes are caused by
agents for which antimicrobials are not effective, e.g., viruses, or by bacteria that must first be cultured to determine their
sensitivity to antimicrobials. A culture, however, is costly and requires several days to receive the test results. Moreover,
most laboratories are unable to detect many of the important bacterial causes of diarrhoea.
Note: Anti-diarrhoeal drugs — including anti-motility agents (e.g., loperamide, diphenoxylate, codeine, tincture of opium),
adsorbents (e.g., kaolin, attapulgite, smectite), live bacterial cultures (e.g., Lactobacillus, Streptococcus faecium),
and charcoal — do not provide practical benefits for children with acute diarrhoea, and some may have dangerous side effects.
These drugs should never be given to children less than 5 years old.
Classification of Persistent Diarrhoea
Persistent diarrhoea is an episode of diarrhoea, with or without blood, which begins acutely and lasts at
least 14 days. It accounts for up to 15 percent of all episodes of diarrhoea but is associated with 30 to 50 percent
of deaths. Persistent diarrhoea is usually associated with weight loss and often with serious non-intestinal infections.
Many children who develop persistent diarrhoea are malnourished, greatly increasing the risk of death. Persistent diarrhoea
almost never occurs in infants who are exclusively breast-fed.
All children with diarrhoea for 14 days or more should be classified based on the presence or absence of any dehydration:
• Children with SEVERE PERSISTENT DIARRHOEA who also have any degree of dehydration require special treatment
and should not be managed at the outpatient health facility.
Referral to a hospital is required. As a rule,treatment of dehydration should be initiated first, unless there is another severe
classification.
• Children with PERSISTENT DIARRHOEA and no signs of dehydration can be safely managed in the outpatient clinic, at least
initially.
Proper feeding is the most important aspect of treatment for most children with
persistent diarrhoea. The goals of nutritional therapy are to: (a) temporarily reduce the amount of
animal milk (or lactose) in the diet; (b) provide a sufficient intake of energy, protein, vitamins and minerals to
facilitate the repair process in the damaged gut mucus and improve nutritional status; (c) avoid giving foods or drinks
that may aggravate the diarrhoea; and (d) ensure adequate food intake during convalescence to correct any malnutrition.
Routine treatment of persistent diarrhoea with antimicrobials is not effective. Some children, however,
have non-intestinal (or intestinal) infections that require specific antimicrobial therapy. The persistent
diarrhoea of such children will not improve until these infections are diagnosed and treated correctly.
Classification of Dysentery
The mother or caretaker of a child with diarrhoea should be asked if there is blood in the stool.
• A child is classified as having DYSENTERY if the mother or caretaker reports blood in the child’s stool.
It is not necessary to examine the stool or perform laboratory tests to diagnose dysentery. Stool culture,
to detect pathogenic bacteria, is rarely possible. Moreover, at least two days are required to obtain the results of a culture.
Although “dysentery” is often described as a syndrome of bloody diarrhoea with fever, abdominal cramps, rectal pain and mucoid
stools, these features do not always accompany bloody diarrhoea, nor do they necessarily define its aetiology or
determine appropriate treatment.
Bloody diarrhoea in young children is usually a sign of invasive enteric infection that carries a substantial risk of serious
morbidity and death. About 10 percent of all diarrhoea episodes in children under 5 years old are dysenteric, but these cause
up to 15 percent of all diarrhoeal deaths.
Dysentery is especially severe in infants and in children who are undernourished, who develop clinically-evident dehydration during
their illness, or who are not breast-fed. It also has a more harmful effect on nutritional status than acute watery diarrhoea.
Dysentery occurs with increased frequency and severity in children who have measles or have had measles in the preceding month,
and diarrhoeal episodes that begin with dysentery are more likely to become persistent than those that start without blood
in the stool.
All children with dysentery (bloody diarrhoea) should be treated promptly with an antibiotic effective against Shigella because:
] (a) bloody diarrhoea in children under 5 is caused much more frequently by Shigella than by any other pathogen; (b) shigellosis
is more likely than other causes of diarrhoea to result in complications and death if effective antimicrobial therapy is not begun
promptly; and (c) early treatment of shigellosis with an effective antibiotic substantially reduces the risk of severe
morbidity or
death.
FEVER
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
All sick children should be checked for fever. Fever is a very common condition and is often the main reason for
bringing children to the health centre. It may be caused by minor infections, but may also be the most obvious sign of a
life-threatening illness, particularly malaria (especially lethal malaria P.falciparum), or other severe infections,
including meningitis, typhoid fever, or measles. When diagnostic capacity is limited, it is important first to identify
those children who need urgent referral with appropriate pre-referral treatment (antimalarial or antibacterial).
Clinical Assessment
Body temperature should be checked in all sick children brought to an outpatient clinic. Children are considered to have fever if
their body temperature is above 37.5°C axillary (38°C rectal). In the absence of a thermometer, children are considered to have
fever if they feel hot. Fever also may be recognised based on a history of fever.
A child presenting with fever should be assessed for:
Stiff neck. A stiff neck may be a sign of meningitis, cerebral malaria or another very severe febrile disease.
If the child is conscious and alert, check stuffiness by tickling the feet, asking the child to bend his/her neck to look down or
by very gently bending the child’s head forward. It should move freely.
Risk of malaria and other endemic infections. In situations where routine microscopy is not available or the results may be delayed,
the risk of malaria transmission must be defined. The World Health Organization (WHO) has proposed definitions of malaria risk
settings for countries and areas with risk of malaria caused by P. falciparum.
A high malaria risk setting is defined as a situation
in which more than 5 percent of cases of febrile disease in children age 2 to 59 months are malarial disease.
A low malarial risk setting is a situation where fewer than 5 percent of cases of febrile disease in children age 2 to 59 months
are malarial disease, but in which the risk is not negligible.
If malaria transmission does not normally occur in the area,
and imported malaria is uncommon, the setting is considered to have no malaria risk. Malaria risk can vary by season.
The national malaria control programme normally defines areas of malaria risk in a country.
If other endemic infections with public health importance for children under 5 are present in the area
(e.g., dengue haemorrhagic fever or relapsing fever), their risk should be also considered.
In such situations, the national health authorities normally adapt the IMCI clinical guidelines locally.
Runny nose. When malaria risk is low, a child with fever and a runny nose does not need an antimalarial.
This child's fever is probably due to a common cold.
Duration of fever. Most fevers due to viral illnesses go away within a few days. A fever that has been present every day for more
than five days can mean that the child has a more severe disease such as typhoid fever. If the fever has been present for more
than five days, it is important to check whether the fever has been present every day.
Measles. Considering the high risk of complications and death due to measles, children with fever should be assessed for signs of
current or previous measles (within the last three months). Measles deaths occur from pneumonia and larynigotracheitis (67 percent),
diarrhoea (25 percent), measles alone, and a few from encephalitis.
Other complications (usually nonfatal) include conjunctivitis,
otitis media, and mouth ulcers. Significant disability can result from measles including blindness, severe malnutrition,
chronic lung disease (bronchiectasis and recurrent infection), and neurologic dysfunction.
Detection of acute (current) measles is based on fever with a generalised rash, plus at least one of the following signs: red eyes,
runny nose, or cough. The mother should be asked about the occurrence of measles within the last three months (recent measles).
Despite great success in improving immunization coverage in many countries, substantial numbers of measles cases and deaths
continue to occur.
Although the vaccine should be given at 9 months of age, immunization often does not take place
(because of false contraindications, lack of vaccine, or failure of a cold chain), or is delayed.
In addition, many measles cases occur early in a child’s life (between 6 and 8 months of age),
especially in urban and refugee populations.
If the child has measles currently or within the last three months, s/he should be assessed for possible complications.
Measles damages the epithelial surfaces and the immune system, and lowers vitamin A levels.
This results in increased susceptibility to infections caused by pneumococcus, gram-negative bacteria, and adenovirus.
Recrudescence of herpes virus, Candida, and malaria can also occur during measles infection.
It is important to check every child with recent or current measles for possible mouth or eye complications.
Other possible complications such as pneumonia, stridor in a calm child, diarrhoea, malnutrition and ear infection are assessed
in relevant sections of the IMCI clinical guidelines.
Before classifying fever, check for other obvious causes of fever (e.g. ear pain, burn, abscess, etc.).
Classification of Fever
• All children with fever and any general danger sign or stiff neck are classified as having
VERY SEVERE FEBRILE DISEASE and should be urgently referred to a hospital after pre-referral treatment
with antibiotics (the same choice as for severe pneumonia or very severe disease).
Note: In areas where malaria P.falciparum is present, such children should also receive a pre-referral dose of an
antimalarial (intramuscular quinine).
Further classifications will depend on the level of malaria risk in the area.
• In a high malaria risk area or season, children with fever and no general danger sign or stiff neck should be
classified as having MALARIA.
Presumptive treatment for malaria should be given to all children who present with fever in the clinic, or who have a
history of fever during this illness. Although a substantial number of children will be treated for malaria when in fact they
have another febrile illness, presumptive treatment for malaria is justified in this category given the high rate of malaria risk
and the possibility that another illness might cause the malaria infection to progress. This recommendation is intended
to maximise
sensitivity, ensuring that as many true cases as possible receive proper antimalarial treatment.
• In a low malarial risk area or season, children with fever (or history of fever) and no general danger sign or stiff neck are classified as having MALARIA and given an antimalarial only if they have no runny nose (a sign of ARI), no measles, and no other obvious cause of fever (pneumonia, sore throat, etc.).
Evidence of another infection lowers the probability that the child's illness is due to malaria. Therefore, children in a low malaria risk area or season, who have evidence of another infection, should not be given an antimalarial.
• In a low malaria risk area or season, children with runny nose, measles or clinical signs of other possible infection are classified as having FEVER — MALARIA UNLIKELY. These children need follow-up. If their fever lasts more than five days, they should be referred for further assessment to determine causes of prolonged pyrexia. If possible, in low malaria risk settings, a simple malaria laboratory test is highly advisable.
• In a no malaria risk area or season an attempt should be made to distinguish cases of possible bacterial infection, which require antibiotic treatment, from cases of non-complicated viral infection. Presence of a runny nose in such situations has no or very little diagnostic value.
When there are obvious causes of fever present — such as pneumonia, ear infection, or sore throat —children could be classified as having POSSIBLE BACTERIAL INFECTION and treated accordingly.
• In a no malaria risk area or season, if no clinical signs of obvious infection are found, the working classification becomes UNCOMPLICATED FEVER.
Such children should be followed up in two days and assessed further. As in other situations, all childrenwith fever lasting more than five days should be referred for further assessment.
Note: Children with high fever, defined as an axillary temperature greater than 39.5°C or a rectal greater than 39°C, should be given a single dose of paracetamol to combat hyperthermia.
Classification of Measles
All children with fever should be checked for signs of current or recent measles (within the last three months) and measles complications.
• SEVERE COMPLICATED MEASLES is present when a child with measles displays any general danger sign, or has severe stomatitis with deep and extensive mouth ulcers or severe eye complications, such as clouding of the cornea. These children should be urgently referred to a hospital.
• Children with less severe measles complications, such as pus draining from the eye (a sign of conjunctivitis) or non-deep and non-extensive mouth ulcers, are classified as MEASLES WITH EYE OR MOUTH COMPLICATIONS. These children can be safely treated at the outpatient facility. This treatment includes oral vitamin A, tetracycline ointment for children with pus draining from the eye, and gentian violet for children with mouth ulcers.Children classified with pneumonia, diarrhoea or ear infection AND measles with eye or mouth complications should be treated for the other classification(s) AND given a vitamin A treatment regimen. Because measles depresses the immune system, these children may be also referred to hospital for treatment.
• If no signs of measles complications have been found after a complete examination, a child is classified as having MEASLES. These children can be effectively and safely managed at home with vitamin A treatment.
EAR PROBLEMS
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
Ear problems are the next condition that should be checked in all children brought to the outpatient health facility. A child presenting with an ear problem should first be assessed for general danger signs, cough or difficult breathing, diarrhoea and fever. A child with an ear problem may have an ear infection. Although ear infections rarely cause death, they are the main cause of deafness in low-income areas, which in turn leads to learning problems .
Clinical Assessment
When otoscopy is not available, look for the following simple clinical signs:
Tender swelling behind the ear. The most serious complication of an ear infection is a deep infection in the mastoid bone. It usually manifests with tender swelling behind one of the child’s ears. In infants, this tender swelling also may be above the ear. When both tenderness and swelling are present, the sign is considered positive and should not be mistaken for swollen lymph nodes.
Ear pain. In the early stages of acute otitis, a child may have ear pain, which usually causes the child to become irritable and rub the ear frequently.
Ear discharge or pus. This is another important sign of an ear infection. When a mother reports an ear discharge, the health care provider should check for pus drainage from the ears and find out how long the discharge has been present.
Classification of Ear Problems
Based on the simple clinical signs above, the child’s condition can be classified in the following ways:
• Children presenting with tenderness and swelling of the mastoid bone are classified as having MASTOIDITIS and should be referred to the hospital for treatment. Before referral, these children first should receive a dose of antibiotic and a single dose of paracetamol for pain.
• Children with ear pain or ear discharge (or pus) for fewer than 14 days are classified as having ACUTE EAR INFECTION and should be treated for five days with the same first-line antibiotic as for pneumonia.
• If there is ear discharge (or pus) for more then 14 days, the child’s classification is CHRONIC EAR INFECTION. Dry the ear by wicking. Generally, antibiotics are not recommended because they are expensive and their efficacy is not proven.
• If no signs of ear infection are found, children are classified as having NO EAR INFECTION and do not require any specific treatment.
CHECKING NUTRITIONAL STATUS — MALNUTRITION AND ANAEMIA
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
After assessing for general danger signs and the four main symptoms, all children should be assessed for malnutrition and anaemia. There are two main reasons for routine assessment of nutritional status in sick children: (1) to identify children with severe malnutrition who are at increased risk of mortality and need urgent referral to provide active treatment; and (2) to identify children with sub-optimal growth resulting from ongoing deficits in dietary intake plus repeated episodes of infection (stunting), and who may benefit from nutritional counselling and resolution of feeding problems. All children also should be assessed for anaemia.
Clinical Assessment
Because reliable height boards are difficult to find in most outpatient health facilities, nutritional status should be assessed by looking and feeling for the following clinical signs:
Visible severe wasting. This is defined as severe wasting of the shoulders, arms, buttocks, and legs, with ribs easily seen, and indicates presence of marasmus.
Oedema of both feet. The presence of oedema (accumulation of fluid) in both feet may signal kwashiorkor. Children with oedema of both feet may have other diseases like nephrotic syndrome. There is a need, however, to differentiate these other conditions in the outpatient settings because referral is necessary in any case.
Weight for age. When height boards are not available in outpatient settings, a weight for age indicator (a standard WHO or national growth chart) helps to identify children with low (Z score less than –2) or very low (Z score less than –3) weight for age who are at increased risk of infection and poor growth and development.
Palmar pallor. Although this clinical sign is less specific than many other clinical signs included in the IMCI guidelines, it can allow health care providers to identify sick children with severe anaemia often caused by malaria infection. Where feasible, the specificity of anaemia diagnosis may be greatly increased by using a simple laboratory test (e.g., the Hb test).
CLASSIFICATION OF NUTRITIONAL STATUS AND ANAEMIA
Using a combination of the simple clinical signs above, children can be classified in one of the following categories:
• Children with SEVERE MALNUTRITION OR SEVERE ANAEMIA (exhibiting visible severe wasting, or severe palmar pallor or oedema of both feet) are at high risk of death from various severe diseases and need urgent referral to a hospital where their treatment (special feeding, antibiotics or blood transfusions, etc.) can be carefully monitored.
• Children with ANAEMIA OR LOW (OR VERY LOW) WEIGHT for age also have a higher risk of severe disease and should be assessed for feeding problems. This assessment should identify common, important problems with feeding that feasibly can be corrected if the caretaker is provided effective counselling and acceptable feeding recommendations based on the child’s age.
When children are classified as having ANAEMIA they should be treated with oral iron. During treatment, the child should be seen every two weeks (follow-up), at which time an additional 14 days of iron treatment is given. If there is no response in pallor after two months, the child should be referred to the hospital for further assessment. Iron is not given to children with severe malnutrition who will be referred. In areas where there is evidence that hookworm, whipworm, and ascaris are the main causes and contributors to anaemia and malnutrition, regular deworming with mebendazole every four to six months is recommended. Mebendazole is inexpensive and safe in young children.
• Children who are not low (or very low) weight for age and who show no other signs of malnutrition are classified as having NO ANAEMIA AND NOT VERY LOW WEIGHT. Because children less than 2 years old have a higher risk of feeding problems and malnutrition than older children do, their feeding should be assessed. If problems are identified, the mother needs to be counselled about feeding her child according to the recommended national IMCI clinical guidelines (see following section).
ASSESSING THE CHILD'S FEEDING
All children less than 2 years old and all children classified as ANAEMIA OR LOW (OR VERY LOW) WEIGHT need to be assessed for feeding.
Feeding assessment includes questioning the mother or caretaker about: (1) breastfeeding frequency and night feeds; (2) types of complimentary foods or fluids, frequency of feeding and whether feeding is active; and (3) feeding patterns during the current illness. The mother or caretaker should be given appropriate advice to help overcome any feeding problems found (for more details, refer to the section on counselling the mother or caretaker).
CHECKING IMMUNIZATION STATUS
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
The immunization status of every sick child brought to a health facility should be checked. Illness is not a contraindication to immunization. In practice, sick children may be even more in need of protection provided by immunization than well children. A vaccine’s ability to protect is not diminished in sick children.
As a rule, there are only four common situations that are contraindications to immunization of sick children:
• Children who are being referred urgently to the hospital should not be immunized. There is no medical contraindication, \but if the child dies, the vaccine may be incorrectly blamed for the death.
Live vaccines (BCG, measles, polio, yellow fever) should not be given to children with immunodeficiency diseases, or to children who are immunosuppressed due to malignant disease, therapy with immunosuppressive agents or irradiation. However, all the vaccines, including BCG and yellow fever, can be given to children who have, or are suspected of having, HIV infection but are not yet symptomatic.
• DPT2/ DPT3 should not be given to children who have had convulsions or shock within three days of a previous dose of DPT. DT can be administered instead of DPT.
• DPT should not be given to children with recurrent convulsions or another active neurological disease of the central nervous system. DT can be administered instead of DPT.
ASSESSING OTHER PROBLEMS
Communicating- History Taking
General Danger Signs
Main Symptoms
Cough or Difficult Breathing
Diarrhoea
Fever
Ear Problems
Nutritional Status
Immunization Status
Other Problems
The IMCI clinical guidelines focus on five main symptoms. In addition, the assessment steps within each main symptom take into account several other common problems. For example, conditions such as meningitis, sepsis, tuberculosis, conjunctivitis, and different causes of fever such as ear infection and sore throat are routinely assessed within the IMCI case management process. If the guidelines are correctly applied, children with these conditions will receive presumptive treatment or urgent referral.
Nevertheless, health care providers still need to consider other causes of severe or acute illness. It is important to address the child’s other complaints and to ask questions about the caretaker’s health (usually, the mother’s). Depending on a specific country’s situation, other unique questions may be raised. For example, in countries where vitamin A deficiency is a problem, sick child encounters should be used as an opportunity to update vitamin A supplementation.
TREATMENT PROCEDURES FOR SICK CHILDREN
IMCI classifications are not necessarily specific diagnoses, but they indicate what action needs to be taken. In the IMCI guidelines, all classifications are colour coded: pink calls for hospital referral or admission, yellow for initiation of treatment, and green means that the child can be sent home with careful advice on when to return. After completion of the assessment and classification procedure, the next step is to identify treatment.
REFERRAL OF CHILDREN AGE 2 MONTHS UP TO 5 YEARS
All infants and children with a severe classification (pink) are referred to a hospital as soon as assessment is completed and necessary pre-referral treatment is administered. Conditions requiring urgent referral.
Note: If a child only has severe dehydration and no other severe classification, and IV infusion is available in the outpatient clinic, an attempt should be made to rehydrate the sick child.
Successful referral of severely ill children to the hospital depends on effective counselling of the caretaker. If s/he does not accept referral, available options (to treat the child by repeated clinic or home visits) should be considered. If the caretaker accepts referral, s/he should be given a short, clear referral note, and should get information on what to do during referral transport, particularly if the hospital is distant.
Urgent Pre-referral Treatments for Children Age 2 Months Up To 5 Years
• Appropriate antibiotic
• Quinine (for severe malaria)
• Vitamin A
• Prevention of hypoglycemia with breastmilk or sugar water
• Oral antimalarial
• Paracetamol for high fever (38.5°C or above) or pain
• Tetracycline eye ointment (if clouding of the cornea or pus draining from eye)
• ORS solution so that the mother can give frequent sips on the way to the hospital
Note: The first four treatments above are urgent because they can prevent serious consequences such as progression of bacterial meningitis or cerebral malaria, corneal rupture due to lack of vitamin A, or brain damage from low blood sugar. The other listed treatments are also important to prevent worsening of the illness.
Non-urgent treatments, e.g., wicking a draining ear or providing oral iron treatment, should be deferred to avoid delaying referral or confusing the caretaker.
If a child does not need urgent referral, check to see if the child needs non-urgent referral for further assessment; for example, for a cough that has lasted more than 30 days, or for fever that has lasted five days or more. These referrals are not as urgent, and other necessary treatments may be done before transporting for referral.
URGENT PRE-REFERRAL TREATMENTS FOR THE SICK CHILD
FROM AGE 2 MONTHS UP TO 5 YEARS
CLASSIFICATION
TREATMENT
For all children before referral:
Prevent low blood sugar by giving breastmilk or sugar water.
DANGER SIGN-CONVULSIONS
If the child is convulsing, give diazepam (10 mg/2 ml solution) in dose 0.1 ml/kg or paraldehyde in dose 0.3 - 0.4 ml/kg rectally; if convulsions continue after 10 minutes, give a second dose of diazepam rectally.
SEVERE PNEUMONIA OR VERY SEVERE DISEASE
Give first dose of an appropriate antibiotic. Two recommended choices are cotrimoxazole and amoxicillin. If the child cannot take an oral antibiotic (children in shock or those who are vomiting incessantly or are unconscious), give the first dose of intramuscular chloramphenicol (40 mg/kg). Options for an intramuscular antibiotic for pre-referral use include benzylpenicillin and ceftriaxone.
VERY SEVERE FEBRILE DISEASE
Give one dose of paracetamol for high fever (38.5°C or above).Give first dose of intramuscular quinine for severe malaria unless no malaria risk.Give first dose of an appropriate antibiotic.
SEVERE COMPLICATED MEASLES
Give first dose of appropriate antibiotic.Give vitamin A.If there is clouding of the cornea or pus draining from the eye, apply tetracycline eye ointment.SEVERE DEHYDRATION WHO Treatment Plan C
If there is no other severe classification, IV fluids should be given in the outpatient clinic according to WHO Treatment Plan C. Give 100 ml/kg IV fluids. Ringer's lactate solution is the preferred commercially available solution. Normal saline does not correct acidosis or replace potassium losses, but can be used. Plain glucose or dextrose solutions are not acceptable for the treatment of severe dehydration.If IV infusion is not possible, urgent referral to the hospital for IV treatment is recommended. When referral takes more than 30 minutes, fluids should be given by nasogastric tube. If none of these are possible and the child can drink, ORS must be given by mouth. Note: In areas where cholera cannot be excluded for patients less than 2 years old with severe dehydration, antibiotics are recommended. Two recommended choices are cotrimoxazole and tetracycline.SEVERE PERSISTENT DIARRHOEA If there is no other severe classification, treat dehydration before referral using WHO Treatment Plan B for some dehydration and Plan C for severe dehydration. Then refer to hospital.
MASTOIDITIS
Give first dose of an appropriate antibiotic. Two recommended choices are cotrimoxazole and amoxicillin. If the child cannot take an oral antibiotic (children in shock or those who are vomiting incessantly or who are unconscious), give the first dose of intramuscular chloramphenicol (40 mg/kg). Options for an intramuscular antibiotic for pre-referral use include benzylpenicillin and ceftriaxone.
Give first dose of paracetamol for pain.
SEVERE MALNUTRITION OR SEVERE ANAEMIA
Give first dose of vitamin A.
TREATMENT IN OUTPATIENT CLINICS
The treatment associated with each non-referral classification (yellow and green) is clearly spelled out in the IMCI guidelines. Treatment uses a minimum of affordable essential drugs (see Figure 5).
ORAL DRUGS
Always start with a first-line drug. These are usually less expensive, more readily available in a given country, and easier to administer. Give a second-line drug (which are usually more expensive and more difficult to obtain) only if a first-line drug is not available, or if the child's illness does not respond to the first-line drug. The health care provider also needs to teach the mother or caretaker how to give oral drugs at home.• Oral antibiotics. The IMCI chart shows how many days and how many times each day to give the antibiotic. Most antibiotics should be given for five days. Only cholera cases receive antibiotics for three days. The number of times to give the antibiotic each day varies (two, three or four times per day). Determine the correct dose of antibiotic based on the child’s weight. If the child’s weight is not available, use the child’s age. Always check if the same antibiotic can be used for treatment of different classifications a child may have. For example, the same antibiotic could be used to treatboth pneumonia and acute ear infection.• Oral antimalarials. Oral antimalarials vary by country. Chloroquine and sulfadoxine-pyrimethamine are the first-line and second-line drugs used in many countries. Chloroquine is given for three days. The dose is reduced o the third day unless the child weighs less than 10 kg. If this is a case, the child should be given the same dose on all three days.•Paracetamol. If a child has a high fever, give one dose of paracetamol in the clinic. If the child has ear pain, give the other enough paracetamol for one day, that is, four doses. Tell her to give one dose every six hours or until the ear pain is gon.• Iron. A child with anaemia needs iron. Give syrup to the child under 12 months of age. If the child is12 months or older, give iron tablets. Give the mother enough iron for 14 days. Tell her to give her child one doe daily for those 14 days. Ask her to return for more iron in 14 days. Also tell her that the iron may make the child's stools black.Note: If a child with some pallor is receiving the antimalarial sulfadoxine-pyrimethamine (Fansidar), do not give iron/folate tablets until a follow-up visit in two weeks. The iron/folate may interfere with the action of the sulfadoxine-pyrimethamine that contains antifolate drugs. If an iron syrup does not contain folate, a child can be given an iron syrup with sulfadoxine-pyrimethamine.• Antihelminth drug. If hookworm or whipworm is a problem in the area, an anaemic child who is 2 years of age or older may need mebendazole. These infections contribute to anaemia because of iron loss through intestinal bleeding. Give 500 mg of mebendazole as a single dose in the clinic.• Vitamin A. Vitamin A is given to a child with measles or severe malnutrition. Vitamin A helps resist the measles virus infection in the eye as well as in the layer of cells that line the lung, gut, mouth and throat. It may also help the immune system to prevent other infections. Vitamin A is available in capsule and syrup form. Use the child's age to determine the dose, and give two doses. Give the first dose to the child in the clinic. Give the second dose to the mother to give her child the next day at home. Every dose of Vitamin A should be recorded because of danger of an overdose.• Safe remedy for cough and cold. There is no evidence that commercial cough and cold remedies are any more effective than simple home remedies in relieving a cough or soothing a sore throat. Suppression of a cough is not desirable because cough is a physiological reflex to eliminate lower respiratory tract secretion. Breastmilk alone is a good soothing remedy.
TREATMENT OF LOCAL INFECTIONS
If the child, age 2 months up to 5 years, has a local infection, the mother or caretaker should be taught how to treat the infection at home.
Instructions may be given about how to:
• Treat eye infection with tetracycline eye ointment;• Dry the ear by wicking to treat ear ifection;• Treat mouth ulcers with gentian violet• Soothe the throat and relieve the cough with a safe remedy.
TREATMENT IN THE OUTPATIENT HEALTH FACILITY OF THE SICK CHILD FROM AGE 2 MONTHS UP TO 5 YEARS
CLASSIFICATION
TREATMENT
PNEUMONIA
Give appropriate antibiotic for five days.
The choice of antibiotic is based on the fact that most childhood pneumonia of bacterial origin is due to Streptococcus pneumoniae or Haemophilus influenzae. The treatment of non-severe pneumonia can utilise a five-day course of either oral cotrimoxazole or amoxicillin. These two oral antibiotics are usually effective treatment for these two bacteria, both are relatively inexpensive, widely available, and are on the essential drug list of most countries. [The advantages of cotrimoxazole are that it is used twice a day, is affordable and compliance is good. It has been shown that with a twice-daily dosing, compliance levels can reach 75 percent or higher. Amoxicillin is almost twice as expensive as cotrimoxazole and standard dosages are usually given three times a day. The compliance with three-times-a-day dosing is about 60 percent or less.]
Soothe the throat and relieve the cough with a safe remedy.
NO PNEUMONIA – COUGH OR COLD
Soothe the throat and relieve the cough with a safe remedy.
SOME DEHYDRATION
WHO Treatment Plan BGive initial treatment with ORS over a period of four hours. The approximate amount of ORS required (in ml) can be calculated by multiplying the child’s weight (in kg) times 75; during these four hours, the mother slowly gives the recommended amount of ORS by spoonfuls or sips. Note: If the child is breast-fed, breast-feeding should continue.After four hours, the child is reassessed and reclassified for dehydration, and feeding should begin; resuming feeding early is important to provide required amounts of potassium and glucose. When there are no signs of dehydration, the child is put on Plan A. If there is still some dehydration, Plan B should be repeated. If the child now has severe dehydration, the child should be put on Plan C.
NO DEHYDRATION
WHO Treatment Plan APlan A focuses on the three rules of home treatment: give extra fluids, continue feeding, and advise the caretaker when to return to the doctor (if the child develops blood in the stool, drinks poorly, becomes sicker, or is not better in three days).Fluids should be given as soon as diarrhoea starts; the child should take as much as s/he wants. Correct home therapy can prevent dehydration in many cases. ORS may be used at home to prevent dehydration. However, other fluids that are commonly available in the home may be less costly, more convenient and almost as effective. Most fluids that a child normally takes can also be used for home therapy especially when given with food. Recommended home fluid should be:
• Safe when given in large volumes. Very sweet tea, soft drinks, and sweetened fruit drinks should be avoided. These are often hyperosmolar owing to their high sugar content (less than 300 mOsm/L). They can cause osmotic diarrhoea, worsening dehydration ad hypenatremia. Also to be avoided are fluids with purgative action and stimulants (e.g., coffee, some medicinal teas or infusions).• Easy to prepare. The recipe should be familiar and its preparation should not require much effort or time. The required ingredients and measuring utensils should be readily available and inexpensive.• Acceptable. The fluid should be one that the mother is willing to give freely to a child with diarrhoea and that the child will readily accept.• Effective. Fluids that are safe are also effective. Most effective are fluids that contain carbohydrates and protein and some salt. However, nearly the same result is obtained when fluids are given freely along with weaning foods that contain salt.
PERSISTENT DIARRHOEA Encourage the mother to continue breastfeeding.If yoghurt is available, give it in place of any animal milk usually taken by the child; yoghurt contains less lactose and is better tolerated. If animal milk must be given, limit it to 50 ml/kg per day; greater amounts may aggravate the diarrhoea.If milk is given, mix it with the child's cereal and do not dilute the milk. At least half of the child's energy intake should come from foods other than milk or milk products. Foods that are hyperosmolar (these are usually foods or drinks made very sweet by the addition of sucrose, such as soft drinks or commercial fruit drinks) should be avoided. They can worsen diarrhoea.Food needs to be given in frequent, small meals, at least six times a day. All children with persistent diarrhoea should receive supplementary multivitamins and minerals (copper, iron, magnesium, zinc) each day for two weeks.
DYSENTERY
The four key elements of dysentery treatment are:
• Antibiotics
• Fluids
• Feeding
• Follow-up
Selection of an antibiotic is based on sensitivity patterns of strains of Shigella isolated in the area (nalidixic acid is the drug of choice in many areas). Recommended duration of treatment is five days. If after two days (during follow-up) there is no improvement, the antibiotic should be stopped and a different one used.
MALARIA
Give an oral antimalarial drug. The selection of first-line and second-line treatment for P.falciparum malaria in endemic countries is an important decision made by health regulating authorities (e.g., Ministry of Health) based on information and technical advise provided by malaria control programes. Generic IMCI guidelines suggest that chloroquine is the first-line and sulfadoxine-pyrimethamine is the second-line antimalarial.
Give one dose of paracetamol for high fever (38.5˚C or above).
FEVER – MALARIA UNLIKELY
POSSIBLE BACTERIAL NFECTION
UNCOMPLICATED FEVER
MEASLES WITH EYE OR MOUTH COMPLICATIONS
Give first dose of Vitamin A. If clouding of cornea or pus draining from the eye, apply tetracycline eye ointment. If mouth ulcers, treat with gentian violet.
MEASLES CURRENTLY (OR WITHIN THE LAST 3 MONTHS)
Give first dose of Vitamin A.
CUTE EAR INFECTION
Give appropriate antibiotic for five days.
Give one dose of paracetamol for pain.
Dry the ear by wicking.
CHRONIC EAR INFECTION
Dry the ear by wicking.
ANAEMIA OR LOW WEIGHT
Assess the child’s feeding and counsel the mother accordingly on feeding.
If pallor is present: give iron; give oral antimalarial if high malaria risk. In areas where hookworm or whipworm is a problem, give mebendazole if the child is 2 years or older and has not had a dose in the previous six months.
NO ANAEMIA AND NOT LOW WEIGHT
If the child is less than 2 years old, assess the child’s feeding and counsel the mother accordingly on feeding.
COUNSELLING A MOTHER OR CARETAKER
A child who is seen at the clinic needs to continue treatment, feeding and fluids at home. The child's mother or caretaker also needs to recognize when the child is not improving, or is becoming sicker. The success of home treatment depends on how well the mother or caretaker knows how to give treatment, understands its importance and knows when to return to a health care provider.
The steps to good communication were listed earlier. Some advice is simple; other advice requires teaching the mother or caretaker how to do a task. When you teach a mother how to treat a child, use three basic teaching steps: give information; show an example; let her practice.
When teaching the mother or caretaker: (1) use words that s/he understands; (2) use teaching aids that are familiar; (3) give feedback when s/he practices, praise what was done well and make corrections; (4) allow more practice, if needed; and (5) encourage the mother or caretaker to ask questions and then answer all questions. Finally, it is important to check the mother’s or caretaker's understanding.
The content of the actual advice will depend on the child’s condition and classifications. Below are essential elements that should be considered when counselling a mother or caretaker:
• Advise to continue feeding and increase fluids during illness;
• Teach how to give oral drugs or to treat local infection;
• Counsel to solve feeding problems (if any);
• Advise when to return.
Advise to continue feeding and increase fluids: The IMCI guidelines give feeding recommendations for different age groups. These feeding recommendations are appropriate both when the child is sick and when the child is healthy. During illness, children’s appetites and thirst may be decreased. However, mothers and caretakers should be counselled to increase fluids and to offer the types of food recommended for the child's age, as often as recommended, even though a child may take small amounts at each feeding. After illness, good feeding helps make up for weight loss and helps prevent malnutrition. When the child is well, good feeding helps prevent future illness.
Teach how to give oral drugs or to treat local infection at home: Simple steps should be followed when teaching a mother or caretaker how to give oral drugs or treat local infections. These steps include: (1) determine the appropriate drugs and dosage for the child's age or weight; (2) tell the mother or caretaker what the treatment is and why it should be given; (3) demonstrate how to measure a dose; (4) describe the treatment steps; (5) watch the mother or caretaker practise measuring a dose; (6) ask the mother or caretaker to give the dose to the child; (7) explain carefully how, and how often, to do the treatment at home; (8) explain that All oral drug tablets or syrups must be used to finish the course of treatment, even if the child gets better; (9) check the mother's or caretaker's understanding.
Counsel to solve feeding problems (if any): Based on the type of problems identified, it is important to give correct advice about the nutrition of the young child both during and after illness. Sound advice that promotes breastfeeding, improved weaning practices with locally appropriate energy- and nutrient-rich foods, and giving nutritious snacks to children 2 years or older, can counter the adverse effect infections have on nutritional status. Specific and appropriate complementary foods should be recommended and the frequency of feeding by age should be explained clearly. Encourage exclusive breastfeeding for the first four months, and if possible, up to six months; discourage use of feeding bottles for children of any age; and provide guidance on how to solve important problems with breastfeeding. The latter includes assessing the adequacy of attachment and suckling. Specific feeding recommendations should be provided for children with persistent diarrhoea. Feeding counselling relevant to identified feeding problems is described in the IMCI national feeding recommendations.
Advise when to return: Every mother or caretaker who is taking a sick child home needs to be advised about when to return to a health facility. The health care provider should (a) teach signs that mean to return immediately for further care; (b) advise when to return for a follow-up visit; and (c) schedule the next well-child or immunization visit.
The table below lists the specific times to advise a mother or caretaker to return to a health facility.A) IMMEDIATELYAdvise to return immediately if the child has any of these signs.Any sick child • Not able to drink or drink or breastfeed• Becomes sicker• Develops a feverIf child has no PNEUONIA: COUGH OR COLD, also return if: • Fast breathin• Difficult breathingIf child has diarrhoea, also return if:
• Blood in stool
• Drinking poorly
B) FOR FOLLOW-UP VISIT
If the child has: Return for follow-up not later than:
PNEUMONIA
DYSENTERY
MALARIA, if fever persists
FEVER MALARIA UNLIKELY or UNCOMPLICATED FEVER, if fever persists
MEASLES WITH EYE OR MOUTH COMPLICATIONS
2 days
PERSISTENT DIARRHOEA
ACUTE EAR INFECTION
CHRONIC EAR INFECTION
FEEDING PROBLEM
ANY OTHER ILLNESS, if not improving
C) NEXT WELL-CHILD VISIT
Advise when to return for the next immunization according to immunization schedule.
FOLLOW-UP CARE
Some sick children will need to return for follow-up care. At a follow-up visit, see if the child is improving on the drug or other treatment that was prescribed. Some children may not respond to a particular antibiotic or antimalarial, and may need to try a second-line drug. Children with persistent diarrhoea also need follow-up to be sure that the diarrhoea has stopped. Children with fever or eye infection need to be seen if they are not improving. Follow-up is especially important for children with a feeding problem to ensure they are being fed adequately and are gaining weight.When a child comes for follow-up of an illness, ask the mother or caretaker if the child has developed any new problems. If she answers yes, the child requires a full assessment: check for general danger signs and assess all the main symptoms and the child's nutritional status.If the child does not have a new problem, use the IMCI follow-up instructions for each specific problem:
• Assess the child according to the instructions;
• Use the information about the child's signs to select the appropriate treatment;
• Give the treatment.
Note: If a child who comes for follow-up has several problems and is getting worse, or returns repeatedly with chronic problems that do not respond to treatment, the child should be referred to a hospital.
The IMCI charts contain detailed instructions on how to conduct follow-up visits for different diseases. Follow-up visits are recommended for sick children classified as having:
• Dysentery
• Malaria, if fever persists
• Fever – Malaria Unlikely, if fever persists
• Measles with eye or mouth complications
• Persistent diarrhoea
• Acute ear infection
• Chronic ear infection
• Feeding problem
• Pallor
• Very low weight for age
• Any other illness, if not improving
OUTPATIENT MANAGEMENT OF YOUNG INFANTS
AGE 1 WEEK UP TO 2 MONTHS
ASSESSMENT OF SICK YOUNG INFANTS
While there are similarities in the management of sick young infants (age 1 week up to 2 months) and children (age 2 months up to 5 years), some clinical signs observed in infants differ from those in older children.
The remainder of this chapter covers instances where the management of young infants differs from that of the small child. For example, it is essential to pay attention to the following clinical signs as an infant’s illness can progress rapidly to death.
Assessment includes the following steps:
• Checking for possible bacterial infection;
• Assessing if the young infant has diarrhoea;
• Checking for feeding problems or low weight;
• Checking the young infant’s immunization status;
• Assessing other problems.
It is important to remember that the guidelines above are not used for a sick new-born who is less than 1 week old. In the first week of life, new-born infants are often sick from conditions related to labour and delivery, or have conditions that require special management. New-borns may be suffering from asphyxia, sepsis from premature ruptured membranes or other intrauterine infection, or birth trauma. Or they may have trouble breathing due to immature lungs. Jaundice also requires special management in the first week of life.
CHECKING FOR MAIN SYMPTOMS
BACTERIAL INFECTION
While the signs of pneumonia and other serious bacterial infections cannot be easily distinguished in this age group, it is recommended that all sick young infants be assessed first for signs of possible bacterial infection.
Clinical Assessment
Many clinical signs point to possible bacterial infection in sick young infants. The most informative and easy to check signs are:
Convulsions (as part of the current illness). Assess the same as for older children.
Fast breathing. Young infants usually breathe faster than older children do. The breathing rate of a healthy young infant is commonly more than 50 breaths per minute. Therefore, 60 breaths per minute is the cut-off rate to identify fast breathing in this age group. If the count is 60 breaths or more, the count should be repeated, because the breathing rate of a young infant is often irregular. The young infant will occasionally stop breathing for a few seconds, followed by a period of faster breathing. If the second count is also 60 breaths or more, the young infant has fast breathing.
Severe Chest indrawing. Mild chest indrawing is normal in a young infant because of softness of the chest wall. Severe chest indrawing is very deep and easy to see. It is a sign of pneumonia or other serious bacterial infection in a young infant.
Nasal flaring (when an infant breathes in) and grunting (when an infant breathes out) are an indication of troubled breathing and possible pneumonia.
A bulging fontanel (when an infant is not crying), skin pustules, umbilical redness or pus draining from the ear are other signs that indicate possible bacterial infection.
Lethargy or unconsciousness, or less than normal movement also indicate a serious condition.
Temperature (fever or hypothermia) may equally indicate bacterial infection. Fever (axillary temperature more than 37.5°C or rectal temperature more than 38°C) is uncommon in the first two months of life. Fever in a young infant may indicate a serious bacterial infection, and may be the only sign of a serious bacterial infection. Young infants can also respond to infection by dropping their body temperature to below 35.5°C (36°C rectal).
Classification of Possible Bacterial Infection
There are two possible classifications for bacterial infection:
• A sick young infant with POSSIBLE SERIOUS BACTERIAL INFECTION is one who has any of the following signs: fast breathing, severe chest indrawing, grunting, nasal flaring, bulging fontanel, convulsions, fever, hypothermia, many or severe skin pustules, umbilical redness extending to the skin, pus draining from the ear, lethargy, unconsciousness, or less than normal movement. This infant should be referred urgently to the hospital after being given intramuscular benzylpenicillin (or ampicillin) plus gentamicin, treatment to prevent hypoglycemia, and advice to the mother on keeping the young infant warm.
• A sick young infant with LOCAL BACTERIAL INFECTION is one who has only a few skin pustules or an umbilicus that is red or draining pus, but without redness extending to the skin. This infant may be treated at home with oral antibiotics but should be seen in follow-up in two days.
DIARRHOEA
All sick young infants should be checked for diarrhoea.
CLINICAL ASSESSMENT AND CLASSIFICATION OF DIARRHOEA
Assessment, classification and management of diarrhoea in sick young infants are similar to those in older children. However, assessing thirst by offering a drink is not reliable, so “drinking poorly” is not used as a sign for the classification of dehydration. In addition, all young infants with persistent diarrhoea or blood in the stool should be referred to the hospital, rather than managed as outpatients
FEEDING PROBLEMS OR LOW WEIGHT
All sick young infants seen in outpatient health facilities should be assessed for weight and adequate feeding, as well as for breast-feeding technique.
Clinical Assessment
Determine weight for age. Assess the same as for older children.Assessment of feeding. Assessment of feeding in young infants is similar to that in older children. It includes three main types of questions about: (1) breastfeeding frequency and night feeds; (2) types of complimentary foods or fluids, frequency of feeding and whether feeding is active or not; and (3) feeding patterns during this illness.If an infant has difficulty feeding, or is breastfed less than 8 times in 24 hours, or taking other foods or drinks, or low weight for age, then breastfeeding should be assessed. Assessment of breastfeeding in young infants includes checking if the infant is able to attach, if the infant is suckling effectively (slow, deep sucks, with some pausing), and if there are ulcers or white patches in the mouth (thrush).
Classification of Feeding Problems or Low Weight
Based on an assessment of feeding and weight, a sick young infant may be classified into three categories:
• NOT ABLE TO FEED – POSSIBLE SERIOUS BACTERIAL INFECTION. The young infant who is not able to feed, or not attaching to the breast or not suckling effectively, has a life-threatening problem. This could be caused by a bacterial infection or another illness. The infant should be referred to a hospital after receiving the same pre-referral treatment as infants with POSSIBLE SERIOUS BACTERIAL INFECTION.
• Infants with FEEDING PROBLEMS OR LOW WEIGHT are those infants who present with feeding problems like not attaching well to the breast, not suckling effectively, getting breastmilk fewer than eight times in 24 hours, receiving other foods or drinks than breastmilk, or those who have low weight for age or thrush (ulcers/white patches in mouth).
Appropriate counselling of the mother should be based on the identified feeding problem: (a) if the infant is not well-attached or not suckling effectively, teach correct positioning and attachment; (b) if the infant is breastfeeding fewer than eight times in 24 hours, advise the mother to increase frequency of feeding; (c) if the infant receives other food or drinks, counsel the mother about breastfeeding more, reducing other foods or drinks, and using a cup; (d) if the mother is not breastfeeding at all, refer for breastfeeding counselling and possible relactation, and advise how to correctly prepare a breastmilk substitute. In infants with thrush, teach the caretaker how to treat thrush at home using gentian violet. Ensure follow-up for any feeding problem or thrush in two days and follow-up low weight for age in 14 days.
• Infants with NO FEEDING PROBLEMS are those who are breastfed exclusively at least eight times in 24 hours and whose weight is not classified as low weight for age according to standard measures.
CHECKING IMMUNIZATION STATUS
As for older children, immunization status should be checked in all sick young infants. Equally, illness is not a contraindication to immunization.Note: Do not give OPV 0 to an infant who is more than 14 days old. If an infant has not received OPV 0 by the time s/he is 15 days old, OPV should be given at age 6 weeks old as OPV 1.
ASSESSING OTHER PROBLEMS
As for older children, all sick young infants need to be assessed for other potential problems mentioned by the mother or observed during the examination. If a potentially serious problem is found or there is no means in the clinic to help the infant, s/he should be referred to hospital.
TREATMENT PROCEDURES FOR SICK INFANTS
REFERRAL OF YOUNG INFANTS AGE 1 WEEK UP TO 2 MONTHS
The first step is to give urgent pre-referral treatment(s). Possible pre-referral treatments include:
• First dose of intramuscular or oral antibiotics
• Keeping the infant warm on the way to the hospital
• Prevention of hypoglycemia with breastmilk or sugar water
• Frequent sips of ORS solution on the way to the hospital
If an infant does not need urgent referral, check to see if the child needs non-urgent referral for further assessment. These referrals are not as urgent. Other necessary treatments may be done before referral.
Figure 6
URGENT PRE-REFERRAL TREATMENTS FOR
SICK YOUNG INFANTS AGE 1 WEEK UP TO 2 MONTHS
CLASSIFICATION
TREATMENT
For all infants before referral:
Prevent low blood sugar by giving breastmilk or sugar water.
Advise mother how to keep the infant warm on the way to the hospital.
CONVULSIONS
If the child is convulsing, give diazepam (10 mg/2 ml solution) in dose 0.1 ml/kg or paraldehyde in dose 0.3 - 0.4 ml/kg rectally; if convulsions continue after 10 minutes, give a second dose of diazepam rectally. Use Phenobarbital ( 200 mg/ml solution) in a dose of 20 mg/kg to control convulsions in infants under 2 weeks of age.
POSSIBLE SERIOUS BACTERIAL INFECTION
AND/ORNOT ABLE TO FEED – POSSIBLE SERIOUS BACTERIAL INFECTION
Give first dose of intramuscular antibiotics. The recommended choices are Gentamicin (2.5 mg/kg) plus benzylpenicillin (50 000 units per kg) OR ceftriaxone OR cefotaxime.SEVERE DEHYDRATION See recommendations for older children, figure 4.DYSENTERY
AND/ORSEVERE PERSISTENT DIARRHOEA See recommendations for older children, figure 4.
TREATMENT IN OUTPATIENT CLINICS
The treatment instructions for a young infant are given in IMCI guidelines. The antibiotics and dosages are different than those for older children. Exceptions are the fluid plans for treating diarrhoea and the instructions for preventing low blood sugar.
WHO Plans A, B, and C and the guidelines on how to prevent low blood sugar are used for young infants as well as older infants and young children.
ORAL DRUGS
The first dose of oral drugs for a young infant should always be given in the clinic. In addition, the mother or caretaker should be taught how to give an oral antibiotic at home. That is, teaching how to measure a single dose, showing how to crush a tablet and mix it with breastmilk, and teaching the treatment schedule. Note: Avoid giving cotrimoxazole to a young infant less than 1 month of age who is premature or jaundiced. Give this infant amoxycillin or benzylpenicillin instead.
TREATMENT OF LOCAL INFECTIONS
There are three types of local infections in a sick young infant that a caretaker can treat at home: an umbilicus that is red or draining pus, skin pustules, or thrush. These local infections are treated with gentian violet.
TREATMENT IN THE OUTPATIENT CLINIC FOR
SICK YOUNG INFANTS FROM 1 WEEK UP TO 2 MONTHS
CLASSIFICATION
TREATMENT
LOCAL BACTERIAL INFECTION
Give an appropriate oral antibiotic. The recommended choices are cotrimoxazole and amoxicillin.Treat local infections and teach the mother to do it at home.SOME DEHYDRATION
NO DEHYDRATION
See recommendations for older children, figure 5.
FEEDING PROBLEM OR LOW WEIGHT
Give appropriate feeding advice.
If thrush, teach the mother to treat thrush at home.
COUNSELLING A MOTHER OR CARETAKER
As with older children, the success of home treatment depends on how well the mother or caretaker knows how to give the treatment, understands its importance, and knows when to return to a health care provider.
Counselling the mother or caretaker of a sick young infant includes the following essential elements:
• Teach how to give oral drugs or to treat local infection.
• Teach correct positioning and attachment for breastfeeding:
a) show the mother how to hold her infant
b) with the infant’s head and body straight
c) facing her breast, with infant’s nose opposite her nipple
d) with infant’s body close to her body
e) supporting infant’s whole body, not just neck and shoulders.
• Show her how to help the infant to attach. She should:
a) touch her infant’s lips with her nipple
b) wait until her infant’s mouth is opening wide
c) move her infant quickly onto her breast, aiming the infant’s lower lip well below the nipple.
• Look for signs of good attachment and effective suckling. If the attachment or suckling is not good, try again.
• Advise about food and fluids: advise to breastfeed frequently, as often as possible and for as long as the infant wants, day and night, during sickness and health.
• Advise when to return:
A) IMMEDIATELY
Advise to return immediately if the infant has any of these signs:
• Breastfeeding or drinking poorly
• Becomes sicker
• Develops a fever
• Fast breathing
• Difficult breathing
• Blood in stool
B) FOR FOLLOW-UP VISIT
If the infant has:
Return for follow-up not later than:
LOCAL BACTERIAL INFECTION
ANY FEEDING PROBLEM
TRUSH
2 days
LOW WEIGHT FOR AGE 14 days
C) NEXT WELL-CHILD VISIT
Advise when to return for the next immunization according to immunization schedule.
FOLLOW-UP CARE
If the child does not have a new problem, use the IMCI follow-up instructions for each specific problem:
• Assess the child according to the instructions;
• Use the information about the child's signs to select the appropriate treatment;
• Give the treatment.
IMCI charts contain detailed instructions on how to conduct follow-up visits for different diseases. Follow-up visits are recommended for young infants who are classified as:• Local bacterial infection
• Feeding problem or low weight (including thrush)
PRINCIPLES OF MANAGEMENT OF
SICK CHILDREN IN A SMALL HOSPITAL
Severely sick children who are referred to a hospital should be further assessed using the expertise and diagnostic capabilities of the hospital setting. However, the first step in assessing children referred to a hospital should be triage — the process of rapid screening to decide in which of the following groups a sick child belongs:
• Those with emergency signs who require immediate emergency treatment: obstructed breathing, severe respiratory distress, central cyanosis, signs of shock, coma, convulsions, or signs of severe dehydration.
• Those with priority signs who should be given priority while waiting in the queue so they can be assessed and treated without delay: visible severe wasting, oedema of both feet, severe palmar pallor, any sick young infant (less than 2 months), lethargy, continual irritability and restlessness, major burns, any respiratory distress, or urgent referral note from another health facility.
• Non-urgent cases that have neither emergency nor priority signs.
Then according to identified priority order, sick children must be examined fully so that no important sign will be missed. The following laboratory investigations need to be available at the small hospital in order to manage sick children:
• Haemoglobin or packed cell volume (PCV)
• Blood smear for malaria
• Blood glucose
• Microscopy of CSF and urine
• Blood grouping and cross-matching
In addition, for sick young infants (under 1 week old), the laboratory investigation for blood bilirubin should be available. Other investigations (such as chest X-ray and stool microscopy) are not considered essential, but could help in complicated cases.
When a child with a severe (pink) classification is admitted to a hospital, a list of possible diagnoses should be drawn up. Remember, a sick child often has more than one diagnosis or clinical problem requiring treatment. The diagnoses in the following table should be considered first for each category.
An appropriate treatment is given to sick children based on the results of the diagnostic procedures and according to the national clinical guidelines. More detailed information about management of children at the first-level referral hospitals may be found in the WHO publication titled Management of the child with a serious infection or severe malnutrition—Guidelines for care at the first-referral level in developing countries (WHO/FCH/CAH/00.1). In addition to describing the most essential treatment procedures, this document outlines the main principles of monitoring the child’s progress. The key aspects in monitoring the progress of a sick child are:
• Devising a monitoring plan. The frequency will depend on the nature and severity of the child’s clinical condition.
• Using a standard chart to record essential information such as correct administration of the treatment, expected progress, possible adverse effects of the treatment, complications that may arise, possible alternative diagnosis.
• Bringing these problems to the attention of senior staff and, if necessary, changing the treatment accordingly.
MAIN SYMPTOMS AND POSSIBLE DIAGNOSES
Unconsciousness, Lethargy or Convulsions
Cough or Difficult Breathing
Diarrhoea Fever
• Meningitis
• Cerebral malaria (only in children exposed to P.falciparum transmission, often seasonal)
• Febrile convulsions (not likely to be cause of unconsciousness)
• Hypoglycaemia (always seek the cause)
• Head injury
• Poisoning
• Shock (can cause lethargy or unconsciousness, but is unlikely to cause convulsions)
• Acute glomerulonephritis with encephalopathy
• Diabetic ketoacidisis
The following are possible diagnoses of young infants referred to the hospital with lethargy:
• Birth asphyxia, hypoxic ischaemic encephalopathy, birth trauma
• Intracranial haemorrhage
• Haemolytic disease of the newborn, kernicterus
• Neonatal tetanus
• Meningitis
• Sepsis
• Pneumonia
• Malaria
• Severe anaemia
• Cardiac failure
• Congenital heart disease
• Tuberculosis
• Pertussis foreign body
• Empyema
• Pneumotorax
• Pneumocystis pneumonia
• Acute watery diarrhoea
• Cholera
• Dysentery
• Persistent diarrhoea
• Diarrhoea with severe malnutrition
• Intussusception
• Malaria
• Septicaemia
• Typhoid
• Urinary tract infection
• HIV infection
• Meningitis
• Otitis media
• Osteomyelitis
• Septic arthritis
• Skin and soft tissue infection
• Pneumonia
• Viral infections
• Throat abscess
• Sinusitis
• Measles• Relapsing fever
• Typhus
• Dengue haemorrhagic fever
Personality Disorder
Overview:
Paranoid Personality Disorder- is evidenced by pervasive distrust and suspiciousness of others.
Schizoid Personality Disorder- is evidenced by social isolation and emotional constriction.
Schizotypal Personality Disorder- is evidenced by social unease, eccentric behavior patterns and cognitive and/or perceptual experiences that cannot be consentually validated.
Antisocial Personality Disorder- is evidenced by the violation of the rights of others or society.
Borderline Personality Disorder- is evidenced by impulsive behavior and unstable social relationships, affect and sense of self and identity.
Histrionic Personality Disorder- is characterized by attention seeking and marked emotionality.
Narcissistic Personality Disorder- is characterized by self centeredness, attention seeking, grandiosity and a lack of empathy.
Avoidant Personality Disorder- is characterized by social constriction, extreme avoidance of negative self evaluation and low self esteem.
Dependent Personality Disorder- is characterized by a clinging and submissive social relationship style and the persistant desire to have ones needs taken care of by others.
Obsessive-Compulsive Personality Disorder- is characterized by the continued need to maintain control, order, neatness, cleanliness, and/or perfectionism.
Cluster A: Odd/Eccentric
The cluster of “odd” personality disorders consists of the paranoid, schizoid, and schizotypal personality disorders.
Extreme suspiciousness, social withdrawal, and peculiar ways of thinking and perceiving things.
Often leave the person isolated, and these people rarely seek treatment
1. Paranoid Personality Disorder
Deeply distrust other people and are suspicious of their motives.
Believes everyone intends them harm.
Avoids close relationships, and their trust in their own ideas and abilities can be excessive.
Critical of weakness and fault in others
.
The oldest of the explanations for this disorder, trace the pattern to early interactions with demanding parents, particularly distant, rigid fathers and overcontrolling, rejecting mothers. Malupit na nanay and wlang paki na tatay.
2. Schizoid Personality Disorder (male)
Disorder persistently avoid contacts and are removed from social relationships and show little in the way of emotion.
“loners”.
Have very weak social skills.
Focus mainly on themselves and are generally unaffected by praise or criticism.
Rarely show any feelings, expressing neither joy nor anger.
They seem to have no need for attention or acceptance
Typically view as cold, humorless, or dull; and generally succeed in being ignored.
Roots in an unsatisfied need for human contact. The parents of people with this disorder are believed to have been unaccepting or even abusive of their children. Manhid na dahil sa pang aabuso nung bata pa.
Due to their lack of ability to hold personal relationships, therapy is ineffective for people with schizoid personality disorder.
Responds stimulation by letting them think about pleasurable experiences or teaching them social skills.
Group therapy is useful with it offers a safe setting for social contact.
2. Schizotypal Personality Disorder (female)
Display a range of interpersonal problems marked by extreme discomfort in close relationships,
Very odd forms of thinking and perceiving, and behavioral eccentricities.
Have great difficulty keeping their attention focused.
Anxious around other, they seek isolation and have few close friends. Many feel intensely lonely.
The disorder is more severe than the paranoid and schizoid personality disorders.
These symptoms may include ideas of reference- beliefs that unrelated event pertain to them in some important way- and bodily illusions, such as sensing an external “force” or presence.
The emotions of these people may be inappropriate, flat, or even humorless. They tend to drift aimlessly and lead an idle, unproductive life.
Linked to poor family communication and to psychological disorders in parents.
Defects in attention and short-term memory may contribute to schizotypal personality disorder. Schizotypal personality disorder to some of the same biological factors as schizophrenia, such as high activity of the neurotransmitter dopamine, enlarged brain ventricles, smaller temporal lobes, and loss of cortical gray matter.
The symptoms of this personality disorder resemble schizophrenia, it has been hypothesized that similar factors are at work in both disorders.
Antipsychotic drugs in small doses have proved helpful in reducing certain unusual thought patterns for patients with this disorder
Cluster b: bad/erratic
1. Borderline Personality Disorder
Characterized by a pattern of instability of interpersonal relationships, affect, and self image, along with marked impulsivity.
More common in women than men.
5 times more common in first degree relatives of borderline patients than in the general population. Many patients with the disorder have histories of childhood abuse.
Tends to have intense relationships, and often alternates between a “black or white” view of the other person.
The patient’s mood is usually dysphoric; chronic anger is frequent. Feeling of emptiness is typical.
Make recurrent suicide attempts, or harm themselves, as by burning with cigarettes or cutting.
Impulsive behaviors include drinking, promiscuity, binge eating or spending. Patients may have brief psychotic like experiences.
Fear of abandonment often precipitates symptoms.
2. Antisocial Personality Disorder
Characterized by a pervasive pattern of disregard for and violation of the rights of others.
Narcissistic and criminal traits.
Prevalence is greatest in early adult years and decreases after that. There is an abrupt drop-off after age 45. Genetic influences
Substance abuse
Criminal behavior
Background of childhood abuse or neglectful parenting Poverty
Attention deficit disorder
Large families
Three to 4 times more common in men than women.
Half of prison populations have antisocial personality disorder.
Exist to satisfy their needs and desires.
Frequently steal, destroy property, cheat, and perform other unlawful acts. They may get sadistic pleasure in their actions.
Interpersonal relationships are expletive, superficial and dishonest.
Patients with antisocial interpersonality disorder are driven by impulsivity and need for excitement. Thus they may drive recklessly, use drugs, and be sexually promiscuous.
Their internal life tends to be shallow and barren. Dpat laging may thrill
3. Histrionic Personality Disorder
Characterized by excessive emotionality and attention-seeking.
Diagnosed more frequently in women, found equally often in men.
Attention-seeking and emotionalism may be culturally determined, which should be taken into account in diagnosis.
There is some evidence of a genetic component, as hysterical traits are more common in relatives of patients with histrionic personality disorder.
Patients with this disorder are uncomfortable if they are not the center of attention.
They draw attention to themselves by being charming, lively, dramatic, or flamboyant.
Inappropriately seductive. They frequently appear to exaggerate their emotions and their degree of intimacy with others. (calling an acquaintance a “very dear friend”).
Their speech can be vague and lacking in detail.
They are easily influenced by people or external events (as, fads), and may excessively trust authority figures (doctors?) To solve all their problems.
4. Narcissistic Personality Disorder
Characterized by a pervasive pattern of grandiosity in fantasy or behavior, a need for admiration and a lack of empathy, present in a variety of contexts.
Background: men than women have the disorder. Little information is available on risk factors or etiology.
Key feature of the disorder is grandiosity and self-importance, which may not be overt.
Expects to be recognized as superior or special, but may not boast of it.
Grandiosity may be expressed in fantasies of success, power, brilliance, or love.
Feel that they are entitled to special
Haughty and arrogant.
Lack sensitivity to the wants and needs of others
Tend to be exploitative in their interpersonal relationships.
Often envious of others or believe that others are envious of them.
They may react to criticism or rejection with disdain or counterattacks on one hand, or with shame and humiliation on the other.
example: this patient is in the waiting room in a loud argument with your clinic staff. He has been waiting since 9 am for a 10:30 appointment, and wants to be seen immediately (it is now 10 am). You dread seeing him because he always takes up excessive amounts of your time because he believes he deserves special attention. He continuously boasts of his business and sexual triumphs. He frequently threatens to “fire” you and to transfer his care to a better doctor.
Cluster C: Fearful/Anxious
1. Dependent Personality Disorder
An excessive need to be taken care of, leading to sub- missive and clinging behavior and fears of separation.
More common in women than in men.
Dependent personality disorder runs in families, and also appears to be genetically related to avoidant personality disorder. Eighty percent of patients with dependent personality disorder have another personality, most often borderline (72%) or avoidant (64%).
Feel inadequate and lack self-confidence; incapable of functioning on their own, depend on others to make their decisions, both major and minor.
They cling to others excessively.
In order to obtain support and nurturance, they subordinate their own needs and desires, and avoid disagreement.
Fear being alone; when one close relationship ends, they seek out another. Because of a sense of inadequacy, it is hard for them to carry out tasks on their own.
Example: a 30 year old woman comes to see you accompanied by her husband. She turns to him for the answers to many of your questions. She never disagrees with him. Later, when you are in the room alone with her discussing a course of treatment, she says “i’ll do anything you think is right, doctor” sang ayon nalang kasi takot iwanan. Walang kusa.
2. Avoidant Personality Disorder
Characterized by social inhibition, feelings of inadequacy and hypersensitivity to negative evaluation.
.men and women are equally affected.
Attributed to an overcritical parental style.
Comorbid with other personality disorders, especially schizoid, schizotypic or dependent personality disorder. Other (axis 1) conditions often comorbid include dysthymia, major depression, social phobia, generalized anxiety disorder, and obsessive compulsive disorder.
Believe themselves to be socially inept, unattractive, or inferior to others.
Fear rejection, criticism or disapproval.
Fear of negative reaction from others
Avoid occupations with significant interpersonal contact, are hesitant to
Become involved in intimate relationships, and are inhibited in new social situations
Want to be sure they will be liked before becoming involved with other people.
Unusually reluctant to take risks or engage in new activities for fear they will prove embarrassing.
. Example: a 55 year old man is being seen by you for angina. He has worked as a mechanic in a small garage for 30 years. He has little customer contact. He is not married, and although he would like to meet women, he says he gets “cold feet” when it comes to going out. He says he doesn’t like being around many people, that they make him “nervous” and “embarrassed”.
3. Obsessive-Compulsive Disorder ( reference: rachel Kaplan)
An anxiety disorder which can afflict a person throughout his lifetime: "the individual who suffers from ocd becomes trapped in a pattern of repetitive thoughts and behaviors that are senseless and distressing but extremely difficult to overcome" .
Obsessions and compulsions are the two main components of this disorder.
Obssession often highly negative such as an ever-present fear of germs.
Compulsions such as repeated handwashings are rituals designed to lessen anxiety produced by obsessions.
Ocd may benefit from medication, behavioral therapy, or a combination of the two.
Behavioral therapy involves teaching the patient "exposure and response prevention techniques": how to deal with obsessions and compulsions without rituals
4. Passive-Aggressive
Characterize by willing but is non-compliant
Nursing Diagnosis:
1. Ineffenctive individual coping
2. Altered personaltiy
3. Disturbance in self-image
Inappropriate range of emotions
Poor impulse control
Skewed perception of other individuals and the environment
Long-standing problems in maintaining healthy relationships
Reduced ability to function in the workplace.
Nursing Management For Personality Disorder:
1. Always use matter of fact especially clients with cluster b because they are manipulative.
2. Behavioral modification / psychotherapy treatment
Transference-based psychotherapy:
Cognitive behavioral therapy, including dialectical behavioral therapy
Social skills training;
Eye movement desensitization and reprocessing (emdr)
*the goal is to stop destructive behavior. The therapist guides the patient to an understanding of the feelings and anxieties that trigger the troublesome conduct establish trust
3. Be consistent
4. Educate client and train for social skill.
Social skills training is used most effectively for patients who experience significant problems in interpersonal relationships.
Learning to start a conversation, shop for food, talk on the phone, and pick up people's behavior cues are important aspects of this treatment..
GASTROINTESTINAL SYSTEM
(DIGESTIVE SYSTEM)
THE GASTROINTESTINAL SYSTEM
OVERVIEW OF ANTOMY AND PHYSIOLOGY:
THE ORGAN OF THE DIGESTIVE SYSTEM ARE GROUPED INTO THE ALIMENTARY CANAL (GI TRACT), CONSISTING OF THE MOUTH, ESOPHAGUS, STOMACH, AND SMALL AND LARGE INTESTINE; AND THE ACCESSORY DIGESTIVE ORGANS, INCLUDING THE LIVER, PANCREAS, GALLBLADDER AND DUCTAL SYSTEM. THE PRIMARY FUNCTIONS OF THIS SYSTEM ARE MOVEMENT OF THE FOOD, DIGESTION, ABSOPTION, ELIMINATION AND PROVISION OF THE CONTINUOUS SUPPLY OF NUTRIENTS, ELECTROLYTES, AND WATER.
☺ MOUTH:
A. CONSISTS OF THE LIPS AND ORAL CAVITY: PROVIDES ENTRANCE AND INITIAL PROCESSING OF THE NUTRIENTS AND SENSORY DATA, SUCH AS TASTE, TEXTURE AND TEMPERATURE.
B. ORAL CAVITY CONTAINS TEETH, USED FOR MASTICATION, AND THE TONGUE, WHICH ASSISTS IN DEGLUTITION, TASTE SENSATION AND MASTICATION.
C. THE SALIVARY GLANDS, LOCATED IN THE MOUTH, PRODUCE SECRETION CONTAINING PTYALIN FOR STARCH DIGESTION AND MUCUS FOR LUBRICANT
D. THE PHARYNX AIDS IN SWALLOWING AND FUNCTION IN INDIGESTION BY PROVIDING TO ROUTE FOR FOOD TO PASS FROM THE MOUTH TO THE ESOPHAGUS
☺ ESOPHAGUS:
MASCMUSCULAR TUBE THAT RECEIVES FOOD FROM THE PHARYNX AND PROPELS IN INTO THE STOMACH BY PERISTALSIS.
☺ STOMACH:
A. LOCATED ON THE LEFT SIDE OF THE ABDOMINAL CAVITY, OCCUPYING THE HYPOCHONDRIAC, EPIGASTRIC, AND UMBILICAL REGIONS.
B. STORES AND MIXES FOOD WITH GASTRIC JUICES AND MUCUS, PRODUCING CHEMICAL AND MECHANICAL CHANGES IN THE BOLUS OF FOOD.
1. THE SECRETION OF DIGESTIVE JUICES IS STIMULATED BY SMELLING, TASTING AND CHEWING FOOD, WHICH IS KNOWN AS THE CEPHALIC PHASE OF DIGESTION.
2. THE GASTRIC PHASE IS STIMULATED BY THE PRESENCE OF FOOD IN THE STOMACH; REGULATED BY NEURAL STIMULATION VIA THE PNS AND HORMONAL STIMULATION THROUGH SECRETIONS OF GASTRIN BY THE GASTRIC MUCOSA.
3. AFTER PROCESSING IN THE STOMACH, THE FOOD BOLUS, CALLED CHIME, IS RELEASE INTO THE SMALL INTESTINE THROUGH THE DUODENUM.
C. TWO SPHINCTERS CONTROL THE RATE OF FOOD PASSAGE:
1. CARDIAC SPHINCTER: LOCATED AT THE OPENING BETWEEN THE ESOPHAGUS AND STOMACH.
2. PYLORIC SPHINCTER: LOCATED BETWEEN THE STOMACH AND DUODENUM.
D. THREE ANATOMIC DIVISIONS: FUNDUS, BODY, AND ANTRUM
E. GASTRIC SECRETIONS:
1. PEPSINOGEN: SECRETED BY CHIEF CELLS, LOCATED IN THE FUNDUS, AIDS IN PROTEIN DIGESTION.
2. HYDROCHLORIC ACID: SECRETED BY PARIETAL CELLS, FUNCTIONS IN PROTEIN DIGESTION, RELEASED IN RESPONSE TO GASTRIC
3. INTRINSIC FACTOR: SECRETED BY PARIETAL CELL, PROMOTES ABSORPTION OF VITAMIN B12.
4. MUCOID SECRETIONS: COAT STOMACH WALL AND PREVENT AUTODIGESTION.
☺ SMALL INTESTINE:
A. COMPOSED OF THE DUODENUM JEJUNUM, AND ILEUM
B. EXTENDS FROM THE PYLORUS TO THE ILEOCECAL VALVE, WHICH REGULATES FLOW INTO THE LARGE INTESTINE AND PREVENTS REFLUX INTO THE SMALL INTESTINE.
C. MAJOR FUNCTION OF SMALL INTESTINE ARE DIGESTION AND ABSORPTION OF THE END PRODUCTS OF DIGESTION.
D. STRUCTURAL FEATURES:
1. VILLI (FUNCTIONAL UNIT OF THE SMALL INTESTINE): FINGERLIKE PROJECTIONS LOCATED IN THE MUCOUS MEMBRANE; CONTAIN GOBLET CELLS THAT SECRETE MUCUS AND ABSORPTIVE CELLS THAT ABSORB DIGESTED FOODSTUFFS.
2. CRYPTS OF LIEBERKUHN: PRODUCE SECRETIONS CONTAINING DIGESTIVE ENZYMES.
3. BRUNNER’S GLANDS: FOUND IN THE SUBMUCOSA OF THE DUODENUM, SECRETS MUCUS.
☺ LARGE INTESTINE:
a. DIVIDED INTO FOUR PARTS: CECUM (WITH APPENDIX), COLON (ASCENDING, TRANSVERSE, DESCENDING, AND SIGMOID), RECTUM, AND ANUS.
b. SERVES AS A RESERVOIR FOR FECAL MATERIAL UNIT DEFECATION OCCURS; FUNCTIONS TO ABSORB WATER AND ELECTROLYTES.
c. MICROORGANISMS PRESENT IN THE LARGE INTESTINE ARE RESPONSIBLE FOR A SMALL AMOUNT OF FURTHER BREAKDOWN AND MAKE SOME VITAMINS.
AMINO ACIDS ARE DEAMINATED BY BACTERIA, RESULTING IN AMMONIA, WHICH IS CONVERTED TO UREA IN THE LIVER.
BACTERIA IN THE LARGE INTESTINE AID IN THE SYNTHESIS OF VITAMIN K AND SOME OF THE VITAMIN B GROUPS.
d. FECES (SOLID WASTE) LEAVE THE BODY VIA THE RECTUM AND ANUS.
ANUS CONTAINS INTERNAL SPHINCTER (UNDER INVOLUNTARY CONTROL) AND EXTERNAL SPHINCTER (VOLUNTARY CONTROL)
FECAL MATTER USUALLY 75% WATER AND 25% SOLID WASTES (ROUGHAGE, DEAD BACTERIA, FAT, PROTEIN, INORGANIC MATTER)
☺ LIVER:
A. LARGEST INTERNAL ORGAN; LOCATED IN THE RIGHT HYPOCHONDRIAC AND EPIGASTRIC REGIONS OF THE ABDOMEN.
B. LIVER LOBULES: FUNCTIONAL UNIT OF THE LIVER, COMPOSED OF HEPATIC CELLS.
C. HEPATIC SINUSOIDS (CAPILLARIES) ARE LINED WITH KUPFFER CELLS, WHICH CARRY OUT THE PROCESS OF PHAGOCYTOSIS.
D. PORTAL CIRCULATION BRINGS BLOOD TO THE LIVER FROM THE STOMACH, SPLEEN, PANCREAS, AND INTESTINES.
E. FUNCTIONS:
1. METABOLISM OF FATS, CARBOHYDRATES, AND PROTEIN; QXIDIZES THESE NUTRIENTS FOR ENERGY AND PRODUCES COMPOUNDS THAT CAN BE STORED.
2. PRODUCTION OF BILE
3. CONJUGATION AND EXCRETION (IN THE FORM OF GLYCOGEN, FATTY ACIDS, MINERALS, FAT-SOLUBLE AND WATER-SOLUBLE VITAMINS) OF BILIRUBIN.
4. STORAGE OF VITAMIN A,D,B12 AND IRON
5. SYNTHESIS OF COAGULATION FACTORS
6. DETOXIFICATION OF MANY DRUGS AND CONJUGATION OF SEX HORMONES.
☺ BILIARY SYSTEM:
CONSISTS OF THE GALLBLADDER AND ASSOCIATED DUCTAL SYSTEM (BILE DUCTS),
A. GALLBLADDER: LIES ON THE UNDERSURFACE OF THE LIVER, FUNCTIONS TO CONCENTRATE AND STORE BILE.
B. DUCTAL SYSTEM: PROVIDES A ROUTE FOR THE BILE TO REACH INTESTINES.
1. BILE IS FORMED IN THE LIVER AND EXCRETED INTO THE HEPATIC DUCT.
2. HEPATIC DUCT JOINS WITH THE CYSTIC DUCT (WHICH DRAINS THE GALLBLADDER) TO FORM THE COMMON DUCT BILE.
3. IF THE SPHINCTER OF THE ODDI IS RELAXED, BILE ENTERS THE DUODENUM. IF CONTRACTED, BILE IS STORED IN THE GALLBLADDER.
☺ PANCREAS:
A. POSITIONED TRANSVERSELY IN THE UPPER ABDOMINAL CAVITY.
B. CONSISTS OF A HEAD, BODY, AND TAIL ALONG WITH A PANCREATIC DUCT, WHICH EXTENDS ALONG THE GLAND AND ENTERS THE DUODENUM VIA THE COMMON BILE DUCT.
C. HAS BOTH EXOCRINE AND ENDOCRINE FUNCTIONS; FUNCTION IN THE GI SYSTEM IS EXOCRINE.
a. EXOCRINE CELLS IN THE PANCREAS SECRETE TRYPSINOGEN AND CHYMOTRYPSIN FOR PROTEIN DIGESTION, AMYLASE TO BREAK DOWN STARCH TO DISACCHARIDES AND LIPASE FOR FAT DIGESTION.
b. ENDOCRINE FUNCTION IS RELATED TO ISLETS OF LANGERHANS.
PHYSIOLOGY OF DIGESTION
AND ABSORPTION:
DIGESTION: PHYSICAL AND CHEMICAL BREAKDOWN OF THE FOOD INTO ABSORPTIVE SUBSTANCE.
a. INITIATED IN THE MOUNTH WHERE FOOD MIXES WITH SALVA AND STARCH IS BROKEN DOWN
b. FOOD THEN PASSES INTO THE ESOPHAGUS WHERE IT IS PROPELLED INTO THE STOMACH.
c. IN THE STOMACH, FOOD IS PROCESSED BY GASTRIC SECRETIONS INTO THE SUBSTANCE CALLED CHYME.
d. IN THE SMALL INTESTINE, CARBOHYDRATES ARE HYDROLYZED TO MONOSACCHARIDES, FATS TO GLYCEROL, AND FATTY ACIDS AND PROTEIN TO AMINO ACIDS TO COMPLETE THE DIGESTIVE PROCESS.
WHEN CHIME ENTERS THE DUODENUM, MUCUS IS SECRETED TO NEUTRALIZE HYDROCHLORIC ACID; IN RESPONSE TO RELEASE OF SECRETIN, PANCREAS RELEASES BICARBONATE TO NEUTRALIZE ACID CHIME.
CHOLECYSTOKININ AND PANCREOZYMIN (CCK-PZ) ARE ALSO PRODUCED BY THE DUODENAL MUCOSA; STIMULATE CONTRACTION OF THE GALLBLADDER ALONG WITH RELAXATION OF THE SPHINCTER OF THE ODDI (TO ALLOW BILE TO FLOW FROM THE COMMON BILE DUCT INTO THE DUODENUM), AND STIMULATE RELEASE OF PANCREATIC ENZYMES.
GLOSSARY
ADVENTITIOUS BREATH SOUNDS
ABNORMAL OR ACQUIRED BREATH SOUNDs
ALOPECIA
THE LOSS OF SCALP HAIR (BALDNESS) OR BODY HAIR
ANGLE OF LOUIS
THE JUNCTION BETWEEN THE BODY OF THE STERNUM AND THE MANUBRIUM; THE STARTING POINT FOR LOCATING THE RIBS ANTERIORLY
ANTIHELIX
THE ANTERIOR CURVE OF THE AURICLE’S UPPER ASPECT
APHASIA
ANY DEFECTS IN OR LOSS OF THE POWER TO EXPRESS ONESELF BY SPEECH, WRITING, OR SIGNS, OR TO COMPREHEND SPOKEN OR WRITTEN LANGUAGE DUE TO DISEASE OR INJURY OF THE CEREBRAL CORTEX
ASTIGMATISM
AN UNEVEN CURVATURE OF THE CORNEA THAT PREVENTS HORIZONTAL AND VERTICAL RAYS FROM FOCUSING ON THE RETINA
AURICLE
FLAP OF THE EAR
AUSCULTATION
THE PROCESS OF LISTENING TO SOUNDS PRODUCED WITHIN THE BODY
BLANCH TEST
A TEST DURING WHICH THE CLIENT’S FINGERNAIL IS TEMPORARILY PINCHED TO ASSESS CAPILLARY REFILL AND PERIPHERAL CIRCULATION
BRUIT
A BLOWING OR SWISHING SOUND CREATED BY TURBULENCE OF BLOOD FLOW
CARIES
TOOTH CAVITIES
CATARACTS
OPACITY OF THE LENS OR CAPSULE OF THE EYE
CERUMEN
THE WAX-LIKE SUBSTANCE SECRETED BY GLANDS IN THE EXTERNAL EAR CANAL
CLUBBING
ELEVATION OF THE PROXIMAL ASPECT OF THE NAIL AND SOFTENING OF THE NAIL BED
COCHLEA
A SEASHELL-SHAPED STRUCTURE FOUND IN THE INNER EAR; ESSENTIAL FOR SOUND TRANSMISSION AND HEARING
CONDUCTION HEARING LOSS
THE RESULT OF INTERRUPTED TRANSMISSION OF SOUND WAVES THROUGH THE OUTER AND MIDDLE EAR STRUCTURES
CONJUNCTIVITIS
INFLAMMATION OF THE BULBAR AND PALPEBRAL CONJUNCTIVA
CREPITATIONS
(1) A DRY, CRACKLING SOUND LIKE THAT OF CRIMPLED CELLOPHANE, PRODUCED BY AIR IN THE SUBCUTANEOUS TISSUE OR BY AIR MOVING THROUGH FLUID IN THE ALVEOLI OF THE LUNGS;
(2) A CRACKLING, GRATING SOUND PRODUCED BY BONE RUBBING AGAINST BONE
CYANOSIS
BLUISH DISCOLORATION OF THE SKIN AND MUCOUS MEMBRANES CAUSED BY REDUCED OXYGEN IN THE BLOOD
DACRYOCYSTITIS
INFLAMMATION OF THE LACRIMAL SAC
DIASTOLE
THE PERIOD DURING WHICH THE VENTRICLES RELAX
DULLNESS
A THUDLIKE SOUND PRODUCED DURING PERCUSSION BY DENSE TISSUE OF BODY ORGANS SUCH AS THE LIVER, SPLEEN, OR HEART
DURATION
THE LENGTH OF TIME THAT A SOUND IS HEARD
EDEMA
THE PRESENCE OF EXCESS INTERSTITIAL FLUID IN THE BODY
ERYTHEMA
EUSTACHIAN TUBE
THE PART OF THE MIDDLE EAR THAT CONNECTS THE MIDDLE EAR TO THE NASOPHARYNX; STABILIZES AIR PRESSURE BETWEEN THE EXTERNAL ATMOSPHERE AND THE MIDDLE EAR
EXOPHTHALMUS
A PROTRUSION OF THE EYEBALLS WITH ELEVATION OF THE UPPER EYELIDS, RESULTING IN A STARTLED OR STARING EXPRESSION
EXTERNAL AUDITORY MEATUS
THE ENTRANCE TO THE EAR CANAL
EXTINCTION
THE FAILURE TO PERCEIVE TOUCH ON ONE SIDE OF THE BODY WHEN TWO SYMMETRIC AREAS OF THE BODY ARE TOUCHED SIMULTANEOUSLY
FASCICULATION
AN ABNORMAL CONTRACTION OR SHORTENING OF A BUNDLE OF MUSCLE FIBERS
FLATNESS
AN EXTREMELY DULL SOUND PRODUCED, DURING PERCUSSION, BY VERY DENSE TISSUE, SUCH AS MUSCLE OR BONE
GINGIVITIS
RED, SWOLLEN GINGIA (GUMS)
GLAUCOMA
A DISTURBANCE IN THE CIRCULATION OF AQUEOUS FLUID; CAUSES AN INCREASE IN INTRAOCULAR PRESSURE
GLOSSITIS
INFLAMMATION OF THE TONGUE
GONIOMETER
A DEVICE USED TO MEASURE THE ANGLE OF A JOINT IN DEGREES
HELIX
THE POSTERIOR CURVE OF THE AURICLE’S UPPER ASPECT
HERNIA
A PROTRUSION (SUCH AS OF THE INTESTINE THROUGH THE INGUINAL WALL OR CANAL)
HORDEOLUM (STY)
A REDNESS, SWELLING, AND TENDERNESS OF THE HAIR FOLLICLE AND GLANDS THAT EMPTY AT THE EDGE OF THE EYELIDS
HYPEROPIA
ABNORMAL REFRACTION IN WHICH LIGHT RAYS FOCUS BEHIND THE RETINA, FARSIGHTEDNESS
HYPERRESONANCE
AN ABNORMAL BOOMING SOUND PRODUCED DURING PERCUSSION OF THE LUNGS
INCUS
THE ANVIL BONE OF THE MIDDLE EAR
INSPECTION
THE VISUAL EXAMINATION I.E. ASSESSING BY USING THE SENSE OF SIGHT
INTENSITY
THE LOUDNESS OR SOFTNESS OF A SOUND, AMPLITUDE
INTENTION TREMOR
INVOLUNTARY TREMBLING WHEN AN INDIVIDUAL ATTEMPTS A VOLUNTARY MOVEMENT
JAUNDICE
A YELLOWISH COLOR OF THE SCLERA, MUCOUS MEMBRANES, AND/OR SKIN
LIFT
AN ABNORMAL ANTERIOR MOVEMENT OF THE CHEST RELATED TO ENLARGEMENT OF THE RIGHT VENTRICLE
LOBULE
EARLOBE
MALLEUS
HAMMER BONE OF THE MIDDLE EAR
MANUBRIUM
THE HANDLELIKE SUPERIOR PART OF THE STERNUM THAT JOINS WITH THE CLAVICLES
MASTOID
A BONY PROMINENCE BEHIND THE EAR
MIOSIS
CONSTRICTED PUPILS
MIXED HEARING LOSS
A COMBINATION OF CONDUCTION AND SENSORINEURAL LOSS
MYDRIASIS
ENLARGED PUPILS
MYOPIA
ABNORMAL REFRACTION IN WHICH LIGHT RAYS FOCUS IN FRONT OF THE RETINA
NORMOCEPHALIC
NORMAL HEAD SIZE
ONE-POINT DISCRIMINATION
THE ABILITY TO SENSE WHETHER ONE OR TWO AREAS OF THE SKIN ARE BEING STIMULATED BY PRESSURE
OSSICLES
THE THREE MIDDLE EAR BONES OF SOUND TRANSMISSION
OTOSCOPE
AN INSTRUMENT USED TO EXAMINE THE EARS
PALLOR
THE ABSENCE OF UNDERLYING RED TONES IN THE SKIN AND MAY BE MOST READILY SEEN IN THE BUCCAL MUCOSA
PALPATION
THE EXAMINATION OF THE BODY USING THE SENSE OF TOUCH
PAROTITIS
INFLAMMATION OF THE PAROTID SALIVARY GLAND
PERCUSSION
THE FORCEFUL STRIKING OF THE CHEST WITH CUPPED HANDS TO LOOSEN SECRETIONS IN THE LUNGS
PERFUSION
PASSAGE OF BLOOD CONSTITUENTS THROUGH THE VESSELS OF THE CIRCULATORY SYSTEM
PERIODONTAL DISEASE
DISORDER OF THE SUPPORTING STRUCTURES OF THE TEETH
PINNA
SEE AURICLE
PITCH
THE FREQUENCY OR NUMBER OF THE VIBRATIONS HEARD DURING AUSCULTATION
PLAQUE
AN INVISIBLE SOFT FILM CONSISTING OF BACTERIA, MOLECULES OF SALIVA, AND REMNANTS OF EPITHELIAL CELLS AND LEUKOCYTES THAT ADHERES TO THE ENAMEL SURFACE OF TEETH
PLEXIMETER
IN PERCUSSION, THE MIDDLE FINGER OF THE DOMINANT HAND PLACED FIRMLY ON THE CLIENT’S SKIN
PLEXOR
IN PERCUSSION, THE MIDDLE FINGER OF THE NON-DOMINANT HAND OR A PERCUSSION HAMMER USED TO STRIKE THE PLEXIMETER
POINT OF MAXIMAL IMPULSE
(PMI) THE POINT WHERE THE APEX OF THE HEART TOUCHES THE ANTERIOR CHEST WALL
PRECORDIUM
AN AREA OF THE CHEST OVERLYING THE HEART
PRESBYOPIA
LOSS OF ELASTICITY OF THE LENS AND THUS LOSS OF ABILITY TO SEE CLOSE OBJECTS AS A RESULT OF THE AGING PROCESS
PROPRIOCEPTORS
SENSORY RECEPTORS THAT ARE SENSITIVE TO MOVEMENT AND THE POSITION OF THE BODY
PYORRHEA
PURULENT PERIODONTAL DISEASE
QUALITY
A SUBJECTIVE DESCRIPTION OF A SOUND (E.G., WHISTLING, GURGLING)
REFLEX
AN AUTOMATIC RESPONSE OF THE BODY TO A STIMULUS
RESONANCE
A LOW-PITCHED, HOLLOW SOUND PRODUCED OVER NORMAL LUNG TISSUE WHEN THE CHEST IS PERCUSSED
RESTING TREMOR
A TREMOR THAT IS APPARENT WHEN THE CLIENT IS AT REST AND DIMINISHES WITH ACTIVITY
S1
THE FIRST HEART SOUND WHICH OCCURS WHEN THE ATRIOVENTRICULAR VALVES (MITRAL AND TRICUSPID) CLOSE
S2
THE SECOND HEART SOUND WHICH OCCURS WHEN THE SEMILUNAR VALVES (AORTIC AND PULMONIC) CLOSE
SEMICIRCULAR CANALS
IN THE INNER EAR; CONTAIN THE ORGANS OF EQUILIBRIUM
SENSORINEURAL HEARING LOSS
THE RESULT OF DAMAGE TO THE INNER EAR, THE AUDITORY NERVE, OR THE HEARING CENTER IN THE BRAIN
SORDES
ACCUMULATION OF FOUL MATTER (FOOD, MICROORGANISMS AND EPITHELIAL ELEMENTS) ON THE TEETH AND GUMS
STAPES
STIRRUPS BONE OF THE MIDDLE EAR
STEREOGNOSIS
THE ABILITY TO RECOGNIZE OBJECTS BY TOUCHING AND MANIPULATING THEM
STERNUM
THE BREASTBONE
SYSTOLE
THE PERIOD DURING WHICH THE VENTRICLES CONTRACT
TARTAR
A VISIBLE, HARD DEPOSIT OF PLAQUE AND DEAD BACTERIA THAT FORMS AT THE GUM LINES
THRILL
A VIBRATING SENSATION OVER A BLOOD VESSEL WHICH INDICATES TURBULENT BLOOD
TRAGUS
THE CARTILAGINOUS PROTRUSION AT THE ENTRANCE TO THE EAR CANAL
TREMOR
AN INVOLUNTARY TREMBLING OF A LIMB OR BODY PART
TRIANGULAR FOSSA
A DEPRESSION OF THE ANTIHELIX
TWO-POINT DISCRIMINATION
SEE ONE-POINT DISCRIMINATION
TYMPANIC MEMBRANE
THE EARDRUM
TYMPANY
A MUSICAL OR DRUMLIKE SOUND PRODUCED DURING PERCUSSION OVER AN AIR FILLED STOMACH AND ABDOMEN
VESTIBULE
CONTAINS THE ORGANS OF EQUILIBRIUM; FOUND IN THE INNER EAR
VISUAL ACUITY
THE DEGREE OF DETAIL THE EYE CAN DISCERN IN AN IMAGE
VISUAL FIELDS
THE AREA AN INDIVIDUAL CAN SEE WHEN LOOKING STRAIGHT AHEAD
VITILIGO
PATCHES OF HYPOPIGMENTED SKIN, CAUSED BY THE DESTRUCTION OF MELANOCYTES IN THE AREA
NORMAL VALUES OF ARTERIAL BLOOD GASES
PH- 7.35–7.45
PAO2 - 80–100 MM HG
PACO2 - 35–45 MM HG
HCO3 - 22–26 MEQ/L
BASE EXCESS _2 TO _2 MEQ/L
O2 SATURATION 95–98%
*SOME NORMAL VALUES WILL VARY ACCORDING TO THE KIND OF TEST CARRIED OUT INTHE LABORATORY.NURSES ARE ADVISED TO USE THE NORMAL VALUES ISSUED BY THEAGENCY WHEN INTERPRETING LABORATORY RESULTS.
INTERPRETING ABGS
1. LOOK AT THE PH:
..A. IF THE PH IS LESS THAN 7.35, THE PROBLEM IS ACIDOSIS.
..B. IF THE PH IS GREATER THAN 7.45, THE PROBLEM IS ALKALOSIS.
2. LOOK AT THE PACO2:
..A. IF THE PACO2 IS LESS THAN 35 MM HG,MORE CARBON DIOXIDE ISBEING EXHALED THAN NORMAL.
..B. IF THE PACO2 IS GREATER THAN 45 MM HG, LESS CARBON DIOXIDEIS BEING EXHALED THAN NORMAL.
3. ASSESS THE PH AND PACO2 RELATIONSHIP FOR A POSSIBLE RESPIRATORYPROBLEM:
..A. IF THE PH IS LESS THAN 7.35 (ACIDOSIS), AND THE PACO2 ISGREATER THAN 45 MM HG, RETAINED CARBON DIOXIDE IS CAUSINGRESPIRATORY ACIDOSIS.
..B. IF THE PH IS GREATER THAN 7.45 (ALKALOSIS), AND THE PACO2 ISLESS THAN 35 MM HG, LACK OF CARBON DIOXIDE IS CAUSING RESPIRATORYALKALOSIS.
4. LOOK AT THE BICARBONATE:
..A. IF THE HCO3 IS LESS THAN 22 MEQ/L, BICARBONATE LEVELS ARELOWER THAN NORMAL.
..B. IF THE HCO3 IS GREATER THAN 26 MEQ/L, BICARBONATE LEVELSARE HIGHER THAN NORMAL.
5. ASSESS PH, HCO3 AND BASE EXCESS (BE) VALUES FOR A POSSIBLEMETABOLIC PROBLEM:
..A. IF THE PH IS LESS THAN 7.35 (ACIDOSIS), THE HCO3 IS LESS THAN22 MEQ/L,AND THE BE IS BELOW _2 MEQ/L, LOW BICARBONATELEVELS ARE CAUSING METABOLIC ACIDOSIS.
..B. IF THE PH IS GREATER THAN 7.45 (ALKALOSIS), THE HCO3 ISGREATER THAN 26 MEQ/L, AND THE BE IS ABOVE _2 MEQ/L,HIGH BICARBONATE LEVELS ARE CAUSING METABOLIC ALKALOSIS.
6. LOOK FOR EVIDENCE OF COMPENSATION:
..A. IN RESPIRATORY ACIDOSIS (PH < 7.35, PACO2 > 45 MM HG), IFTHE HCO3 IS GREATER THAN 26 MEQ/L, THE KIDNEYS ARE RETAININGBICARBONATE TO MINIMIZE THE ACIDOSIS: RENAL COMPENSATION.
..B. IN RESPIRATORY ALKALOSIS (PH > 7.45, PACO2 < 35 MM HG), IFTHE HCO3 IS LESS THAN 22 MEQ/L, THE KIDNEYS ARE EXCRETINGBICARBONATE TO MINIMIZE THE ALKALOSIS: AGAIN, RENALCOMPENSATION.
..C. IN METABOLIC ACIDOSIS (PH < 7.35,HCO3_ < 22 MEQ/L),IF THEPACO2 IS LESS THAN 35 MM HG, CARBON DIOXIDE IS BEING“BLOWN OFF” TO MINIMIZE THE ACIDOSIS: RESPIRATORY COMPENSATION.
..D. IN METABOLIC ALKALOSIS (PH > 7.45, HCO3 > 26 MEQ/L), IFTHE PACO2 IS GREATER THAN 45 MM HG, CARBON DIOXIDE IS BEINGRETAINED TO COMPENSATE FOR EXCESS BASE: AGAIN, RESPIRATORYCOMPENSATION.
TEACHING: HOME CARE<
FLUID, ELECTROLYTE, AND ACID–BASE BALANCE
MONITORING FLUID INTAKE AND OUTPUT
■ TEACH THE CLIENT AND FAMILY AS APPROPRIATE HOW TO MONITOR FLUIDINTAKE AND OUTPUT, INCLUDING USING A COMMODE OR COLLECTIONDEVICE (“HAT”) IN THE TOILET, EMPTYING AND MEASURING URINARYCATHETER DRAINAGE, COUNTING OR WEIGHING DIAPERS.
■ INSTRUCT THE CLIENT AND FAMILY TO MONITOR WEIGHT ON A REGULARBASIS AT THE SAME TIME OF DAY,USING THE SAME SCALE AND WITH THECLIENT WEARING THE SAME AMOUNT OF CLOTHING.
■ INFORM THE CLIENT AND FAMILY WHEN TO CONTACT A HEALTH CARE PROFESSIONAL,SUCH AS IN THE CASES OF A SIGNIFICANT CHANGE IN URINEOUTPUT; ANY CHANGE OF 5 POUNDS OR MORE IN A 1- TO 2-WEEK PERIOD;PROLONGED EPISODES OF VOMITING, DIARRHEA, OR INABILITY TOEAT OR DRINK; DRY, STICKY MUCOUS MEMBRANES; EXTREME THIRST;SWOLLEN FINGERS, FEET, ANKLES, OR LEGS; DIFFICULTY BREATHING, SHORTNESSOF BREATH, RAPID HEARTBEAT; AND CHANGES IN BEHAVIOR ORMENTAL STATUS.
MAINTAINING FOOD AND FLUID INTAKE
■ INSTRUCT THE CLIENT AND FAMILY ABOUT ANY DIET OR FLUID RESTRICTIONS,SUCH AS A LOW-SODIUM DIET.CONTACT A DIETITIAN TO PROVIDEAPPROPRIATE TEACHING.
■ TEACH FAMILY MEMBERS THE IMPORTANCE OF OFFERING FLUIDS REGULARLYTO CLIENTS WHO ARE UNABLE TO MEET THEIR OWN NEEDS BECAUSEOF AGE, IMPAIRED MOBILITY OR COGNITION, OR OTHER CONDITIONSSUCH AS IMPAIRED SWALLOWING DUE TO A STROKE.
■ IF THE CLIENT IS ON ENTERAL OR INTRAVENOUS FLUIDS AND FEEDING ATHOME, TEACH CAREGIVERS ABOUT PROPER ADMINISTRATION AND CARE.CONTACT A HOME HEALTH OR HOME INTRAVENOUS SERVICE TO PROVIDESERVICES AND TEACHING.
SAFETY
■ INSTRUCT THE CLIENT TO CHANGE POSITIONS SLOWLY IF APPROPRIATE,ESPECIALLYWHEN MOVING FROM A SUPINE TO A SITTING OR STANDING POSITION.
■ INFORM THE CLIENT AND FAMILY ABOUT THE IMPORTANCE OF GOODMOUTH AND SKIN CARE. TEACH THE CLIENT TO CHANGE POSITIONS FREQUENTLYAND TO ELEVATE THE FEET ON A STOOL WHEN SITTING FOR ALONG PERIOD.
■ TEACH THE CLIENT AND FAMILY HOW TO CARE FOR INTRAVENOUS ACCESSSITES OR GASTRIC TUBES. INCLUDE WHAT TO DO IF TUBES BECOMEDISLODGED.
MEDICATIONS
■ EMPHASIZE THE IMPORTANCE OF TAKING MEDICATIONS ASPRESCRIBED.
■ INSTRUCT CLIENTS TAKING DIURETICS TO TAKE THE MEDICATION IN THEMORNING. IF A SECOND DAILY DOSE IS PRESCRIBED, THEY SHOULD TAKEIT IN THE LATE AFTERNOON TO AVOID DISRUPTING SLEEP TO URINATE.
■ INFORM CLIENTS ABOUT ANY EXPECTED SIDE EFFECTS OF PRESCRIBEDMEDICATIONS AND HOW TO HANDLE THEM (E.G., IF A POTASSIUMDEPLETINGDIURETIC IS PRESCRIBED, INCREASE INTAKE OF POTASSIUMRICHFOODS; IF TAKING A POTASSIUM-SPARING DIURETIC, AVOID EXCESSPOTASSIUM INTAKE SUCH AS USING A SALT SUBSTITUTE).
■ TEACH CLIENTS WHEN TO CONTACT THEIR PRIMARY CARE PROVIDER, FOREXAMPLE, IF THEY ARE UNABLE TO TAKE A PRESCRIBED MEDICATIONOR HAVE SIGNS OF AN ALLERGIC OR TOXIC REACTION TO A MEDICATION.MEASURES SPECIFIC TO CLIENT’S PROBLEM
■ PROVIDE INSTRUCTIONS SPECIFIC TO THE CLIENT’S FLUID, ELECTROLYTE, ORACID–BASE IMBALANCE, SUCH AS
A. FLUID VOLUME DEFICIT
B. RISK FOR FLUID VOLUME DEFICIT
C. FLUID VOLUME EXCESS
REFERRALS
■ MAKE APPROPRIATE REFERRALS TO HOME HEALTH OR COMMUNITY SOCIALSERVICES FOR ASSISTANCE WITH RESOURCES SUCH AS MEALS, MEALPREPARATION AND FOOD, INTRAVENOUS INFUSIONS AND ACCESS, ENTERALFEEDINGS, AND HOMEMAKER OR HOME HEALTH AIDE SERVICESTO HELP WITH ADLS.
COMMUNITY AGENCIES AND OTHER SOURCES OF HELP
■ PROVIDE INFORMATION ABOUT COMPANIES OR AGENCIES THAT CANPROVIDE DURABLE MEDICAL EQUIPMENT SUCH AS COMMODES, LIFTCHAIRS, OR HOSPITAL BEDS FOR PURCHASE, FOR RENTAL, OR FREE OFCHARGE.
■ PROVIDE A LIST OF SOURCES FOR SUPPLIES SUCH AS CATHETERS ANDDRAINAGE BAGS,MEASURING DEVICES, TUBE FEEDING FORMULAS, ANDELECTROLYTE REPLACEMENT DRINKS.
■ SUGGEST ADDITIONAL SOURCES OF INFORMATION AND HELP SUCH ASTHE AMERICAN DIETETIC ASSOCIATION, THE AMERICAN HEARTASSOCIATION, AND THE AMERICAN LUNG ASSOCIATION
TEACHING: CLIENT CARE
SKIN PROBLEMS AND CARE
DRY SKIN
■ USE CLEANSING CREAMS TO CLEAN THE SKIN RATHER THAN SOAP ORDETERGENT, WHICH CAUSE DRYING AND, IN SOME CASES, ALLERGICREACTIONS.
■ USE BATH OILS,BUT TAKE PRECAUTIONS TO PREVENT FALLS CAUSED BYSLIPPERY TUB SURFACES.
■ THOROUGHLY RINSE SOAP OR DETERGENT, IF USED, FROM THE SKIN.
■ BATHE LESS FREQUENTLY WHEN ENVIRONMENTAL TEMPERATURE ANDHUMIDITY ARE LOW.
■ INCREASE FLUID INTAKE.
■ HUMIDIFY THE AIR WITH A HUMIDIFIER OR BY KEEPING A TUB OR SINKFULL OF WATER.
■ USE MOISTURIZING OR EMOLLIENT CREAMS THAT CONTAIN LANOLIN, PETROLEUMJELLY, OR COCOA BUTTER TO RETAIN SKIN MOISTURE.
SKIN RASHES
■ KEEP THE AREA CLEAN BY WASHING IT WITH A MILD SOAP. RINSE THESKIN WELL, AND PAT IT DRY.
■ TO RELIEVE ITCHING, TRY A TEPID BATH OR SOAK. SOME OVER-THECOUNTERPREPARATIONS, SUCH AS CALADRYL LOTION,MAY HELP BUTSHOULD BE USED WITH FULL KNOWLEDGE OF THE PRODUCT.
■ AVOID SCRATCHING THE RASH TO PREVENT INFLAMMATION, INFECTION,AND FURTHER SKIN LESIONS.
■ CHOOSE CLOTHING CAREFULLY. TOO MUCH CAN CAUSE PERSPIRATIONAND AGGRAVATE A RASH.
ACNE
■ WASH THE FACE FREQUENTLY WITH SOAP OR DETERGENT AND HOT WATERTO REMOVE OIL AND DIRT.
■ AVOID USING OILY CREAMS,WHICH AGGRAVATE THE CONDITION.
■ AVOID USING COSMETICS THAT BLOCK THE DUCTS OF THE SEBACEOUSGLANDS AND THE HAIR FOLLICLES.
■ NEVER SQUEEZE OR PICK AT THE LESIONS.THIS INCREASES THE POTENTIALFOR INFECTION AND SCARRING.
TEACHING: HOME CARE
SKIN INTEGRITY
MAINTAINING INTACT SKIN
■ DISCUSS RELATIONSHIP BETWEEN ADEQUATE NUTRITION (ESPECIALLYFLUIDS,PROTEIN, VITAMINS B AND C, IRON, AND CALORIES) ANDHEALTHY SKIN.
■ DEMONSTRATE APPROPRIATE POSITIONS FOR PRESSURE RELIEF.
■ ESTABLISH A TURNING OR REPOSITIONING SCHEDULE.
■ DEMONSTRATE APPLICATION OF APPROPRIATE SKIN PROTECTIONAGENTS AND DEVICES.
■ INSTRUCT TO REPORT PERSISTENT REDDENED AREAS.
■ IDENTIFY POTENTIAL SOURCES OF SKIN TRAUMA AND MEANS OFAVOIDANCE.
PROMOTING WOUND HEALING
■ DISCUSS IMPORTANCE OF ADEQUATE NUTRITION (ESPECIALLY FLUIDS,PROTEIN, VITAMINS B AND C, IRON, AND CALORIES).
■ INSTRUCT IN WOUND ASSESSMENT AND PROVIDE MECHANISM FORDOCUMENTING.
■ EMPHASIZE PRINCIPLES OF ASEPSIS, ESPECIALLY HAND WASHINGAND PROPER METHODS OF HANDLING USED DRESSINGS.
■ PROVIDE INFORMATION ABOUT SIGNS OF WOUND INFECTION ANDOTHER COMPLICATIONS TO REPORT.
■ REINFORCE APPROPRIATE ASPECTS OF PRESSURE ULCER PREVENTION.
■ DEMONSTRATE WOUND CARE TECHNIQUES SUCH AS WOUND CLEANSINGAND DRESSING CHANGING.
■ DISCUSS PAIN CONTROL MEASURES, IF NEEDED.
TEACHING: CLIENT CARE
BREAST SELF-EXAMINATION
INSPECTION BEFORE A MIRROR
LOOK FOR ANY CHANGE IN SIZE OR SHAPE; LUMPS OR THICKENINGS; ANYRASHES OR OTHER SKIN IRRITATIONS; DIMPLED OR PUCKERED SKIN; ANY DISCHARGEOR CHANGE IN THE NIPPLES (E.G., POSITION OR ASYMMETRY).
INSPECT THE BREASTS IN ALL OF THE FOLLOWING POSITIONS:
■ STAND AND FACE THE MIRROR WITH YOUR ARM RELAXED AT YOUR SIDESOR HANDS RESTING ON THE HIPS; THEN TURN TO THE RIGHT AND THE LEFTFOR A SIDE VIEW (LOOK FOR ANY FLATTENING IN THE SIDE VIEW).
■ BEND FORWARD FROM THE WAIST WITH ARMS RAISED OVER THE HEAD.
■ STAND STRAIGHT WITH THE ARMS RAISED OVER THE HEAD AND MOVETHE ARMS SLOWLY UP AND DOWN AT THE SIDES. (LOOK FOR FREEMOVEMENT OF THE BREASTS OVER THE CHEST WALL.)
■ PRESS YOUR HANDS FIRMLY TOGETHER AT CHIN LEVEL WHILE THE ELBOWSARE RAISED TO SHOULDER LEVEL.
PALPATION: LYING POSITION
■ PLACE A PILLOW UNDER YOUR RIGHT SHOULDER AND PLACE THE RIGHTHAND BEHIND YOUR HEAD.THIS POSITION DISTRIBUTES BREAST TISSUEMORE EVENLY ON THE CHEST.
■ USE THE FINGER PADS (TIPS) OF THE THREE MIDDLE FINGERS (HELD TOGETHER)ON YOUR LEFT HAND TO FEEL FOR LUMPS.
■ PRESS THE BREAST TISSUE AGAINST THE CHEST WALL FIRMLY ENOUGH TOKNOW HOW YOUR BREAST FEELS. A RIDGE OF FIRM TISSUE IN THE LOWERCURVE OF EACH BREAST IS NORMAL.
■ USE SMALL CIRCULAR MOTIONS SYSTEMATICALLY ALL THE WAY AROUNDTHE BREAST AS MANY TIMES AS NECESSARY UNTIL THE ENTIRE BREASTIS COVERED. (REVIEW FIGURES 28–70 THROUGH 28–72 IN CHAPTER28 FOR PATTERNS THAT THE CLIENT MAY USE.)
■ BRING YOUR ARM DOWN TO YOUR SIDE AND FEEL UNDER YOUR ARMPIT,WHERE BREAST TISSUE IS ALSO LOCATED.
■ REPEAT THE EXAM ON YOUR LEFT BREAST, USING THE FINGER PADS OFYOUR RIGHT HAND.
PALPATION: STANDING OR SITTING
■ REPEAT THE EXAMINATION OF BOTH BREASTS WHILE UPRIGHT WITHONE ARM BEHIND YOUR HEAD.THIS POSITION MAKES IT EASIER TOCHECK THE AREA WHERE A LARGE PERCENTAGE OF BREAST CANCERS AREFOUND, THE UPPER OUTER PART OF THE BREAST AND TOWARD THEARMPIT.
■ OPTIONAL: DO THE UPRIGHT BSE IN THE SHOWER. SOAPY HANDS GLIDEMORE EASILY OVER WET SKIN.REPORT ANY CHANGES TO YOUR HEALTH CARE PROVIDER PROMPTLY
SURGICAL HAND SCRUB
. A FIVE (5) MINUTE ANATOMICAL TIMED SCRUB WILL BE USED FOR ALL SURGICAL HAND SCRUBS.
. FINGERNAILS MUST BE FREE OF POLISH/ENAMEL AND OF MEDIUM LENGTH.
. NO JEWELRY IS PERMITTED ON THE HANDS AND ARMS WHILE PERFORMING AS A MEMBER OF THE SURGICAL TEAM.
**REMEMBER TO PUT YOUR MASK ON PRIOR TO STARTING YOU SCRUB.**
. WASH HANDS AND ARMS WITH SOLUTION TO 2 INCHES ABOVE THE ELBOW.
. CLEAN FINGERNAILS WITH FILE. TAKE STERILE BRUSH IN RIGHT HAND. WET BRUSH WITH WATER AND SOAP. SCRUB FINGERNAILS OF LEFT HAND.
. START SCRUBBING FINGERS OF LEFT HAND, ONE AT A TIME, TREATING EACH FINGER AS FOUR-SIDED; PALM, KNUCKLES, AND BACK OF HAND. REPEAT WITH RIGHT HAND.
. SCRUB RIGHT WRIST AND CONTINUE UP ARM TO 2 INCHES ABOVE ELBOW. REPEAT WITH LEFT ARM. DISCARD BRUSH. RINSE BOTH HANDS AND ARMS UNDER RUNNING WATER KEEPING HANDS ABOVE LEVEL OF ELBOW SO THAT WATER RUNS OFF THE ELBOWS AND NOT THE HANDS.
GLOVING PROCEDURE - OPEN
. AVOID CONTACT OF STERILE GLOVES WITH UNGLOVED HANDS DURING CLOSED-GLOVE PROCEDURE.
. FOR CLOSED-GLOVE METHOD, NEVER LET THE FINGERS EXTEND BEYOND THE STOCKINETTE CUFF DURING THE PROCEDURE. CONTACT WITH UNGLOVED FINGERS CONSTITUTES CONTAMINATION OF THE GLOVE.
. FOR OPEN-GLOVE METHOD, TOUCH ONLY THE CUFF OF THE GLOVE WITH UNGLOVED HAND, AND THEN ONLY GLOVE TO GLOVE FOR OTHER HAND.
. IF CONTAMINATION OCCURS DURING EITHER PROCEDURE, BOTH GOWN AND GLOVES MUST BE DISCARDED AND NEW GOWN AND GLOVES MUST BE ADDED.
. WHEN REMOVING GLOVES AFTER A PROCEDURE IS FINISHED, THE GLOVES ARE REMOVED AFTER THE GOWN IS REMOVED INSIDE OUT, USING GLOVE-TO-GLOVE, THEN SKIN-TO-SKIN TECHNIQUE.
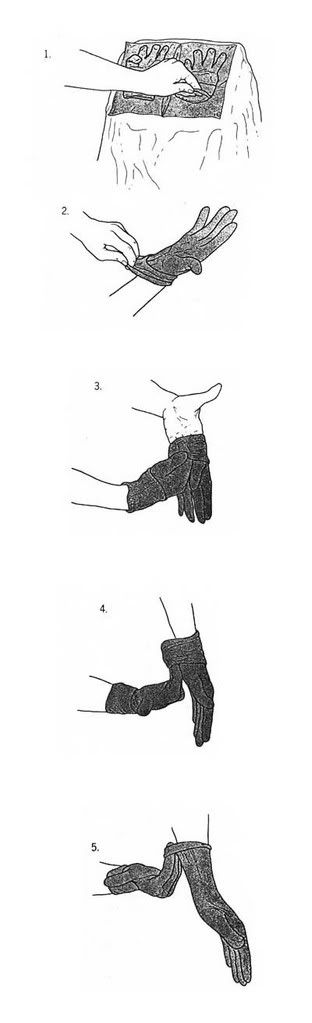
PROCEDURE FOR SURGICAL GOWNING AND GLOVING
PURPOSE: TO MAINTAIN STERILITY WHEN DONNING GOWN AND GLOVES.
EQUIPMENT:
STERILE GLOVES
STERILE GOWNS
STERILE TOWELS
NURSING ACTION:
PROCEDURE STEPS:
DRYING HANDS AND ARMS
REACH DOWN TO THE OPENED STERILE PACKAGE AND PICK UP THE TOWEL. BE CAREFUL NOT TO DRIP WATER ONTO THE PACK. BE SURE NO ONE IS WITHIN ARMS REACH. SCRUB NURSE (OR TECHNICIAN) PREPARING TO GOWN REMOVES THE HAND TOWELON TOP OF THE GOWN FROM THE OPENED GOWN PACKAGE.
OPEN THE TOWEL FULL-LENGTH, HOLDING ONE END AWAY FROM NON-STERILE SCRUB ATTIRE. BEND SLIGHTLY FORWARD TO AVOID TOWEL TOUCHING ATTIRE.
DRY BOTH HANDS THOROUGHLY, BUT INDEPENDENTLY. TO DRY ONE ARM, HOLD THE TOWEL IN THE OPPOSITE HAND AND, USING AN OSCILLATING MOTION OF THE ARM, DRAW THE TOWEL UP TO THE ELBOW.
CAREFULLY REVERSE THE TOWEL, STILL HOLDING IT AWAY FROM THE BODY. DRY THE OPPOSITE ARM ON THE UNUSED END OF THE TOWEL.
KEYPOINT: AFTER SCRUBBING, THE HANDS AND ARMS SHOULD BE THOROUGHLY DRIED BEFORE THE STERILE GOWN IS DONNED TO PREVENT STRIKE THROUGH OF ORGANISMS FROM WET SKIN.
.GOWNING FOR CLOSED GLOVE METHOD.
REACH DOWN TO THE STERILE PACKAGE AND LIFT THE FOLDED GOWN DIRECTLY UPWARD.
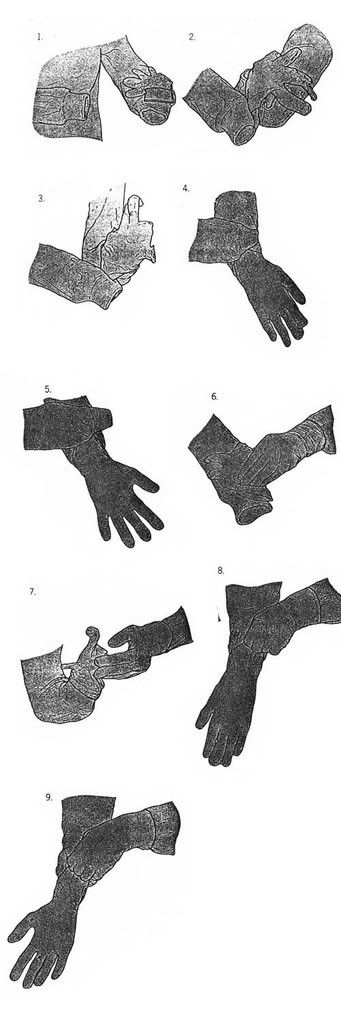
KEYPOINT: THE ENTIRE GOWN USED BY SCRUB PERSON IS STERILE PRIOR TO DONNING.
STEP BACK AWAY FROM THE TABLE, INTO AN UNOBSTRUCTED AREA TO PROVIDE A WIDE MARGIN OF SAFETY WHILE GOWNING.
HOLDING THE FOLDED GOWN, CAREFULLY LOCATE THE NECKBAND.
HOLDING THE INSIDE FRONT OF THE GOWN JUST BELOW THE NECKBAND WITH BOTH HANDS, LET THE GOWN UNFOLD, KEEPING THE INSIDE OF THE GOWN TOWARD THE BODY. DO NOT TOUCH THE OUTSIDE OF THE GOWN WITH BARE HANDS.
HOLDING THE HANDS AT SHOULDER LEVEL, SLIP BOTH ARMS INTO THE ARMHOLES SIMULTANEOUSLY.
THE CIRCULATING NURSE BRINGS THE GOWN OVER THE SHOULDER BY REACHING INSIDE THE SHOULDER AND ARMS SEAMS. THE GOWN IS PULLED ON, LEAVING THE SLEEVES EXTENDED OVER THE HANDS. THE BACK OF THE GOWN IS SECURELY TIED OR FASTENED AT THE NECK AND WAIST TOUCHING OUTSIDE OF GOWN AT THE LINE OF TIES OR FASTENERS, IN BACK ONLY.
IF THE GOWN IS WRAP-AROUND STYLE, THE STERILE FLAP TO COVER THE BACK IS NOT TOUCHED UNTIL THE PERSON HAS GOWNED AND GLOVED.
IF THE TOP OF THE GOWN DROPS DOWNWARD INADVERTENTLY, DISCARD THE GOWN AS CONTAMINATED. NEVER REVERSE A PIECE OF STERILE LINEN IF THE WRONG END IS DROPPED TOWARD THE FLOOR.
KEYPOINT: ONCE DONNED, THE STERILITY OF THE FOLLOWING AREAS IS MAINTAINED:
THE GOWN IS CONSIDERED STERILE IN FRONT FROM CHEST TO TABLE OR WAIST LEVEL.
THE SLEEVES ARE CONSIDERED STERILE TO TWO INCHES ABOVE THE ELBOW.ALL OTHER AREAS OF THE GOWN ARE CONSIDERED CONTAMINATED. THE NECKLINE, SHOULDERS, AREAS UNDER THE ARM AND BACK OF THE GOWN ARE CONSIDERED UNSTERILE.
THE BACK OF A WRAP-AROUND "STERILE-BACK" IS NOT CONSIDERED STERILE.
THE STOCKINETTE CUFF IS NOT CONSIDERED STERILE AND MUST BE COVERED BY GLOVES
GLOVING BY CLOSED GLOVE METHOD
USING THE LEFT HAND, AND KEEPING IT WITHIN THE CUFF OF THE LEFT SLEEVE, PICK UP THE RIGHT GLOVE, FROM THE INNER WRAP OF THE GLOVE PACKAGE, BY GRASPING THE FOLDED CUFF.
KEYPOINT: THE CLOSED GLOVE METHOD IS TO BE USED BY ANYONE WHO GOWNS AND GLOVES THEMSELVES.
EXTEND THE RIGHT FOREARM WITH PALM UPWARD. PLACE THE PALM OF GLOVE AGAINST THE PALM OF THE RIGHT HAND, GRASPING IN THE RIGHT HAND THE TOP EDGE OF THE CUFF, ABOVE THE PALM. IN CORRECT POSITION GLOVE FINGERS ARE POINTING TOWARD YOU AND THE THUMB SIDE OF THE GLOVE IS DOWN.
GRASP THE BACK OF THE CUFF IN THE LEFT HAND AND TURN IT OVER THE END OF THE RIGHT SLEEVE AND HAND. THE CUFF OF THE GLOVE IS NOW OVER THE STOCKINETTE CUFF OF THE GOWN, WITH THE HAND STILL INSIDE THE SLEEVE.
GRASP THE TOP OF THE RIGHT GLOVE AND UNDERLYING GOWN SLEEVE WITH COVERED LEFT HAND. PULL THE GLOVE ON OVEREXTENDED RIGHT FINGERS UNTIL THE GLOVE COMPLETELY COVERS THE STOCKINETTE CUFF.
GLOVE THE LEFT HAND IN THE SAME MANNER, REVERSING HANDS, USE THE GLOVED RIGHT HAND TO PULL ON THE LEFT GLOVE.
KEYPOINT: AFTER HANDS ARE GLOVED, WIPE POWDER OFF OUTSIDE OF GLOVES WITH A DAMP TOWEL TO AVOID SEEDING WOUND WITH POTENTIAL SOURCE OF GLOVE POWDER GRANULOMA.
ONCE STERILE GLOVES ARE DONNED, THE STERILE FLAP IS TURNED TO COVER THE SCRUB'S BACK. THE DISPOSABLE GOWNS HAVE THE END OF ONE TIE COVERED BY A DISPOSABLE STRIP. HAND STRIP TO CIRCULATOR, TAKING CARE TO PROTECT HANDS. TURN AROUND TOWARD OPPOSITE SIDE, THEREBY CLOSING GOWN. GRASP THE TIE AT A DISTANCE FROM THE END. THE CIRCULATOR PULLS THE STRIP, RELEASING IT FROM THE STILL-STERILE END OF THE TIE, AND DISCARDS IT. TIE THE TIES AT FRONT OR SIDE OF THE GOWN AS INDICATED.
KEYPOINT: THE SCRUB IS CAREFUL TO NOT DROP THE OTHER STRIP TO PREVENT BREAK IN TECHNIQUE.
.GOWNING ANOTHER PERSON.
OPEN THE HAND TOWEL AND LAY IT ON THE SURGEON’S HAND, BEING CAREFUL NOT TO TOUCH THE HAND.
UNFOLD THE GOWN CAREFULLY, HOLDING IT AT THE NECKBAND.
KEEPING HANDS ON THE OUTSIDE OF THE GOWN UNDER A PROTECTIVE CUFF OF THE NECK AND SHOULDER AREA, OFFER THE INSIDE OF THE GOWN TO THE SURGEON. HE/SHE SLIPS THE ARMS INTO THE SLEEVES.
RELEASE THE GOWN. THE SURGEON HOLDS ARMS OUTSTRETCHED WHILE THE CIRCULATING NURSE PULLS THE GOWN ONTO THE SHOULDERS AND ADJUSTS THE SLEEVES SO THAT THE CUFFS ARE PROPERLY PLACED. IN DOING SO, ONLY THE INSIDE OF THE GOWN IS TOUCHED AT THE SEAMS.
GLOVING ANOTHER PERSON
PICK UP THE RIGHT GLOVE, GRASP IT FIRMLY, WITH FINGERS UNDER EVERTED CUFF. HOLD THE PALM OF THE GLOVE TOWARD THE SURGEON.
STRETCH THE CUFF SUFFICIENTLY FOR THE SURGEON TO INTRODUCE THE HAND. AVOID TOUCHING THE HAND BY HOLDING YOUR THUMBS OUT.
EXERT UPWARD PRESSURE AS THE SURGEON PLUNGES THE HAND INTO THE GLOVE.
UNFOLD THE EVERTED GLOVE CUFF OVER THE CUFF OF THE SLEEVE.
REPEAT FOR THE LEFT HAND.
AFTER GOWNING AND GLOVING COMPLETED
SITTING OR LEANING AGAINST A NONSTERILE SURFACE IS A BREAK IN TECHNIQUE. IF THE STERILE TEAM SITS TO OPERATE, THEY DO SO WITHOUT PROXIMITY TO NONSTERILE AREAS.
NEVER LEAVE ROOM AFTER YOU ARE GOWNED AND GLOVED FOR A SPECIFIC CASE. DO NOT CAUSE CROSS CONTAMINATION BY WEARING GOWN AND GLOVES IN HALLS OR TO VISIT OTHER ROOMS.
CHANGING GOWN DURING OPERATION
IF GLOVE IS CONTAMINATED, LET CIRCULATOR REMOVE GOWN, THEN GLOVES.
GRASP THE RIGHT SHOULDER OF THE LOOSENED GOWN WITH THE LEFT HAND AND PULL THE GOWN DOWNWARD FROM THE SHOULDER AND OFF THE RIGHT ARM, TURNING THE SLEEVE INSIDE OUT.
TURN THE OUTSIDE OF THE GOWN AWAY FROM THE BODY WITH FLEXED ELBOWS.
GRASP THE LEFT SHOULDER WITH THE RIGHT HAND AND REMOVE THE GOWN ENTIRELY, PULLING IT OFF INSIDE OUT.
DISCARD THE GOWN IN A TRASH RECEPTACLE IF DISPOSABLE.
KEYPOINT: THE GOWN IS ALWAYS REMOVED INSIDE OUT TO PROTECT THE ARMS AND SCRUB SUIT FROM THE CONTAMINATED OUTSIDE OF THE GOWN. THE GOWN IS ALWAYS REMOVED BEFORE THE GLOVES TO PROTECT THE HANDS FROM THE CONTAMINATED GOWN.
CHANGING GLOVE DURING OPERATION
KEYPOINT: THE CLOSED GLOVE TECHNIQUE CANNOT BE USED FOR GLOVE CHANGE DURING AN OPERATION WITHOUT CONTAMINATION OF THE NEW GLOVE BY THE SLEEVE OF THE GOWN OR WITHOUT CONTAMINATION OF THE HAND BY THE CUFF OF THE GOWN. THE CUFF MUST NOT BE PULLED DOWN OVER HAND.
TURN AWAY FROM THE STERILE FIELD.
EXTEND THE CONTAMINATED HAND TO THE CIRCULATOR WHO GRASPS THE OUTSIDE OF THE GLOVE CUFF ABOUT 2 INCHES BELOW THE TOP OF THE GLOVE AND PULLS THE GLOVE OFF INSIDE OUT.
PREFERABLY A STERILE TEAM MEMBER GLOVES ANOTHER. IF THIS IS NOT POSSIBLE, STEP ASIDE AND GLOVE THE HAND USING THE OPEN GLOVE TECHNIQUE.
.REMOVING GOWN AND GLOVES AFTER CASE.
GOWNS AND GLOVES ARE TO BE REMOVED IN THE OPERATING ROOM AT THE END OF THE CASE.
THE GOWN IS ALWAYS REMOVED BEFORE THE GLOVES. IT IS PULLED DOWNWARD FROM THE SHOULDERS, TURNING THE SLEEVES INSIDE OUT AS IT IS PULLED OFF THE ARMS. SEE VIII ABOVE FOR DETAILS.)
WHEN REMOVING GLOVES, GRASP THE CUFF OF THE LEFT GLOVE WITH THE GLOVED FINGERS OF THE RIGHT HAND AND PULLIT OFF INSIDE OUT.
SLIP THE UNGLOVED FINGERS OF THE LEFT HAND UNDER THE CUFF OF THE RIGHT GLOVE AND SLIP IT OFF INSIDE OUT.
DISCARD THE GLOVES IN A TRASH RECEPTACLE.
WASH HANDS.
KEYPOINT: GLOVES ARE REMOVED USING "GLOVE TO GLOVE" AND "SKIN TO SKIN TECHNIQUE" TO AVOID CONTAMINATING THE HANDS.
NURSING CONCEPTS
FUNCTIONAL CONCEPTS ON PRIORITIZING
. OXYGENATION- CARDIOVAXULAR, RESPIRATORY
. FLUIDS & NUTRITION- ENDOCRINE, GASTRO
. MOBILITY- NEURO, MUSCULOSKELETAL
. ELIMINATION- RENAL, GASTRO
. METABOLISM- ENDOCRINE, RENAL, NEURO
DISEASE CONCEPTS
ABDOMINAL AORTIC ANEURYSM:
. PREDISPOSING FX- HYPERTENSION
. S/SX- PULSATING ADBL PAIN
. LOW BACK PAIN
. AUSCULTAION OF BRUIT
. INC BP ON UPPER EX
. DEC BP ON LOWER EX
. NSG RESP- PROMOTE CIRCULATION
. CHECK FOR DISTAL PULSES
ABRUPTIO PLACENTA:
. ASSESS FOR (+) HOMAN'S SIGN(+) CHVOSTEKS SIGN
. RISK FX- TRAUMA (PREGNANT ON VA)
. DARK PAINFUL BLEEDING
. DX- UTZ
. NSG RESPONSIBILITY- PREVENTION OF SHOCK
. MGT- EMERGENCY CS
. FLUID AND ELECTROLYTES (FLUID RETENTION)
PLACENTA PREVIA:
. MATERNAL AGE IS ABOVE 35
. DX- UTZ
. PAINLESS BLEEDING
. NSG RESP- POS'N PT ON SEMI-FOWLERS
ACROMEGALY:
. LARGE SIZE SHOES
. INC IN BLD SUGAR LEVEL
. CONDITION IS IRREVERSIBLE
. MEDICATION- PARLODEL
ACUTE GLUMERULONEPHRITIS:
. PERIORBITAL EDEMA
. NSG DX- IMPAIRED SKIN INTEGRITY
. URINE- COLA OR TEA COLORED URINE
. DIET- LOW CHON, LOW NA
NEPHROTIC SYNDROME:
. PERI AND GENERALIZED EDEMA
. DIET- LOW NA, HIGH CHON
. STERIODS SHOULD BE TAKEN WITH MEALS
ACUTE LYMPHOCYTIC LEUKEMIA:
. S/SX -EASY FATIGABILITY
. HIGH RISK FOR MULTIPLE INFXN
. DEC IN URIC ACID
. NSG RESP- PALCE PT IN A PRIVATE ROOM, REVERSE ISOLATION
AIDS:
. HIGH RISK FOR OPPOTUNISTIC INFXN EG PNEUMONIA, LYMPH MAST
. MEDICATION- CHEMOTHERAPHY
. TEST- (+) MANTOUX TEST 5 MM INDURATION
. NSG RESP- PLACE PT IN PRIVATE ROOM
. DO NOT RECAP NEEDLE
ADDISONS DSE:
. DECREASE ADRECORTICAL HORMONES
. RISK FX- INFXN
. NOTE FOR CHANGES IN SKIN COLOR- BRONZE LIKE COLORED SKIN
. PT WILL EXHIBIT- HYPOTENSION (NSG RESP CHECK BP), DEC NA LEVEL, DEC SUGAR LEVEL, DEC SEX HORMONE LEVEL
. PLACE PT IN A FLUID RESUSCITATION
. MEDICATION IS LIFETIME
. DIET-HIGH NA, LOW K
AGORAPHOBIA:
. FEAR OF OPEN SPACES
. PT HAS CONQUERED PHOBIA IF- WALKS TO THE MAILBOX, SPENDS TIME IN THE YARD, GOES TO THE MALL
ALCOHOLISM
. HYPOTENSION (ALCOHOL TOXICITY)
. WITHDRAWAL ONSET- 12 HRS ALFTER LAST INTAKE
. JAUNDICE (HEPATIC SYND)
ALZHEIMERS DSE:
. AFFECTATION- COGNITIVE
. GOAL OF CARE- REORIENTATION & FUNCTIONAL ACTIVITIES
. MEDICATION- COGNEX (ARICEF) GIVEN AT NIGHT
. NSG RESP- FOCUS SHOLD BE ON TX
AMNIOTIC FLUID EMBOLISM:
. ANAPHYLACTIC SYNDROME OF PREGNANCY
. RX FX-ABRUPTIO PLACENTA
. S/SX- CHAEST PAIN AND DYSPNEA (DUE TO AMNIOTIC FLUID)
ANEMIA PERNICIOUS:
. (+) PAIN
. RED TONGUE (GLOSITIS)
. TEST- SCHILLING TEST (24 HR URINE)
. TX- VIT B12 INJECTION (LIFETIME)
. COMPLICATION- PERIPHERAL NEURITIS ON DISTAL PARTS (ARMS AND LEGS)
ANOREXIA:
. PERFECTIONIST PARENTS
. AMENORRHEA (3 MOS)
. FINE HAIR ( LANUGO LIKE)
BULIMIA:
. BINGE AND PURGE ( BINGE EATING THEN VOMITING)
ANTISOCIAL:
. HABITUAL BREAKING OF LAW
. EG - A THIEF WOULD ALWAYS BE A THIEF
APNEA IN INFANT:
. CESSATION OF BREATHING FOR MORE THAN 20 SEC
. ELECTRODES SHOULD BE ON THE EXTERNAL AREA
. DX PROCEDURE- EEG, ECG, POLYSONOGRAPHY
. SWEAT CHLORIDE TEST IS NOT INDICATED
APPENDICITIS:
. RLQ PAIN
. RAPTURED APPY- WHEN PAIN SUBSIDES
ARTHRITIS, RHEUMATIOD:
. INC IN ESR
ARTHRITIS GOUT:
. DIET- LOW PURINE DIET (ORGAN MEATS)
. NSG RESP- PROVIDE BED CRADLE
. INC FLUDI INTAKE
ARTHRITIS, OSTEO:
. RISK FX- TRAUMA & FRACTURE
. S/SX- LOCAL JOINT PAIN
. NSG DX- PAIN
ASTHMA:
. DO NOT MEDICATE WITH- PROPANOLOL, ASPIRIN, CHAMOMILE
ADHD:
. MED- RITALIN (GIVEN EARLY AM AFTER MEAL)
. 6 HRS BEFORE BEDTIME
. NSG PRIORITY- NUTRITION & SAFETY
AUTONOMIC DYSREFLEXIA:
. RISK FX- FULL BLADDER
. S/SX- INC BP, DIAPHORESIS
. NSG RESP- KEEP RET CATH @ BEDSIDE
. ABSOLUTE UPRIGHT POS'N
BATTERED WIFE SYNDROME:
. PRIORITY SHELTER
. PROVIDE CRISIS HOTLINE
. SUPPORT CLIENT
BENIGN PROSTATIC HYPERTROPHY:
. S/SX- FREQ, URGENCY, HESITANCY OF URINATION
. DEC SIZE AND FROCE OF URINATION
. MGT- PREINEAL PROSTATECTOMY
BIPOLAR DISORDER:
. MED- LITHIUM ( INC FLUID AND NA INTAKE)
. THERA LEVEL- .8 MEQ/DL
. LITHIUM PROMOTES GI DISTURBANCE
BLEEDING ESOPHAGEAL VARICES:
. COFFEE GROUND OUTPUT
. MGT- BALLOON TAMPONAGE (SENGSTAKEN-BAKEMORE TUBE)
. KEEP SCISSORS @ BEDSIDE
BRONCHOILITIS:
. CAUSATIVE AGENT- RESP VIRUS
. INTERVENTION- HAND WASHING, ANTI-VIRAL AGENT, ENSURE AIRWAY
BRONCHOGENIC CANCER:
. CHANGING & NAGGING COUGH
. KEEP AIRWAY OPEN
BORDERLINE PERSONALITY DISORDER:
. IMPULSIVITY
. SUICIDAL
. HISTRIONIC-WANTS TO BE THE CENTER OF ATTN
BUERGER'S DSE:
. AVOID SMOKING
. COMPLICATION- THROMBOS FORM'N
. NSG PRIORITY- PREVENTION OF THROMBUS FORM'N
RAYNUAD'S DSE:
. AFFECTATION- ARTERIES
. DIMINISHING HAIR IN THE EX
CANCER, BLADDER:
. PAINLESS HEMATURIA
. RISK FX- SMOKING, GENETIC DISPOSITION
CANCER, BREAST:
. LATERAL IDENTATION IN BREAST
. GENETIC LINK
. BREAST ASSYMETRY
. MAMOGRAPHY- THE ENTIRE BREAST ON THE PLATE
. BREAST SELF EXAM EVERY MONTH AFTER MENS
CANCER, CERVIX:
. CAUSE- HERPES, MULTIPARITY
. CANCER OF ESOPHAGUS
. S/SX- DYSPHAGIA
. COMPLICATION OF RADIATION THERA- HYERSALIVATION
CANCER, ESOPHAGUS:
. ALCOHOLIC
. LECTURERS
. SINGERS
CANCER, PROSTATE:
. VAGUE ABD'L DISCOMFORT
. INC ACID PHOSPATASE
CANDIADIASIS:
. WHITISH DISCHARGE
. ORAL CANDIDIASIS- IMPAIRED SWALLOWING
CARDIAC TAMPONADE:
. MUFFLED HEART SOUNDS
. DILATED NECK VEINS
. HYPOTENSION
CATARACT:
. PAINLESS BLURRING OF VISION
. POST OF AVOID STRAINING, BENDING, LIFTING OF HEAVY OBJECTS
CELIACS DSE:
. DIET- GLUTEN FREE (NO WHEAT BREAD)
. DSE CONDITION IS LIFETIME
. DX- GLUTEN CHALLENGE TEST
CEREBROVASCULAR DISORDER:
. NSG DX- UNILATERAL NEGLECT
. KEEP SUCTION MACHINE @ BEDSIDE
CHEST INJURY:
. PARADOXICAL CHEST MOVEMENT
. POSITION PT ON AFFECTED SIDE
CHICKEN POX:
. AVOID ASPIRIN ( RAYS SYNDROME)
CHILD ABUSE:
. BRUISES ON BACK AND LOWER EX
. NSG RESP- REPORT TO AUTHORITY
CHOLECYSTITIS:
. RUQ RADIATING TO THE SHOULDER PAIN
CHLAMYDIA:
. CAN LEAD TO STERILITY IF RECURRENT
CHROHNS DSE:
. HYPERACTIVE BOWEL SOUNDS
CLEFT LIP:
. MEDICINE DROPPER WHEN FEEDING
. PLACE PT ON SUPINE AFTER FEEDING
CLEFT PALATE:
. USE CUP WHEN FEEDING
. POSITON PT ON PRONE
. NSG RESP POST OP- ELBOW RESTRAINT
*IF CLEFT LIP & PALATE- POS'N PATE ON SIDE LYING
COPD:
. PURSED LIP BREATHING
. S/SX- DISTENDED NECK, RUQ TENDERNESS, EDEMA
COMPLETE HEART BLOCK:
. MED- ATROPINE SO4
. NSG DX- ALTERED TISSUE PERFUSION
. COMPLICATION- HEART FAILURE
CONGESTIVE HEART FAILURE:
. LEFT SIDED- DYSPNEA
. RIGHT SIDED- DISTENDED NECK VEINS
. MED- MORPHINE (DEC VENOUS RETURN TO THE HEART)
CRETINISM:
. MANIFESTATION- APATHY
. PT ON SPECIAL EDUCATION
. END RESULT- MENTAL RETARDATION
CROUP:
. MAINTAIN AIRWAY PATENCY
. KEEP TRACH @ BEDSIDE
. PLACE PT ON MIST TENT
CUSHINGS SYNDROME:
. S/SX- THIN FRAGILE SKIN, FACIAL HAIR
. TRUNKAL OBESITY
. METABOLLIC ALKALOSIS
. PT IS PRONE TO DELAYED WOUND HEALING
. HYPERGLYCEMIA
. CHECK BLD SUGAR
CYSTIC FIBROSIS (HIRSPRUNG DSE):
. AUTOSOMAL RECESSIVE (GENETICALLY TRANSMITTED)
. POLYPHAGIA
. REFER TO GENETICIST
. AFFECTATION- MECONIUM ILEUS
. SALTY BABY
. 25% POSSIBLITY OF INHERITANCE OF BOTH PARENT ARE CARRIER
CYSTITIS:
. PRIMARY COMPLICATION- CYTOTOXIC
. RISK FX- BUBBLE BATH
. ENCOURAGE INC FLUID INTAKE
DELIRIUM TREMENS:
. COARSE TREMORS
. PROVIDE WELL LIGHTED ROOM
DEPRESSION, POST PARTUM:
. S/SX- INSOMIA, DEC LIBIDO
. LAST FOR 2 WEEKS POST PARTUM, BEYOND TWO WEEKS CONSIDER PSYCHOSIS
. PROVIDE DIM LIGHTED ROOM
DEPRESSION, CHILDHOOD:
. SOCIAL DISOCIATION
. PLAYS ALONE @ SCHOOL YARD
DEPRESSION ADULT:
. FATIGUE AND CONSTIPATION
. WATCH OUT FOR SUICIDAL INTENT IF PT APPEARS CHEERFUL TWO WEEKS AFTER
DEPRESSION, ELDERLY:
. HIGH RISK FOR INJURY SELF INFLICTED
. MOSTLY ON PT WITH CHRONIC DSE
DIABETES, GESTATIONAL:
. GOAL OF CARE- MAINTAIN SUGAR @ 70-110 MG/DL
DIABETES, CHILDHOOD (JUVENILE):
. S/SX- FREQUENT TRIPS TO CR
DIABETES INSIPIDUS:
. POLYDIPSIA
. OLIGURIA - TEST FOR URINE SPECIFIC GRAVITY
. TX- DESMOPRESSIN (NASALLY)
DIABETES MELLITUS:
. RISK FX - OVER WEIGHT(30%)
. DIABETIC KETOACIDOSIS- RAPID DEEP BREATHING (KAUSMAUL)
. EXCESSIVE THIRST
DIVERTICULITIS:
. ELEVATED WBC
. ENCOURAGE DEC FIBER INTAKE
DUCHENES MUSCULAR DYSTROPHY:
. CHECK FOR RESPIRATION (GOWER SIGN)
. EMG IS INDICATED
. REFER PT TO - RT, PT, GENTICIST,
. X LINK RECESSIVE
DUMPING SYNDROME:
. INTERVENTION- LIE DOWN AFTER MEAL
. INCREASE FAT INTAKE
. DSE IS NOT LIFETIME
. FLUIDS SHOULD BE TAKEN ONLY BET MEALS
ECTOPIC PREGNANCY:
. INTERMITTENT STABBING KNIFE LIKE ABDOMNAL PAIN
. SHARP & INTERMITTENT CRAMPY PAIN & DULL
EPILEPSY:
. SAFETY AND AIRWAY
. ANTICONVULSANT
EXPRESSIVE APHASIA:
. USE PICTURE BOARDS
. PROVIDE PT ADEQ TIME WHEN REPLYING
RECEPTIVE APHASIA:
. TALK TO PT SLOWLY
GERD:
. NEXIUM
. HEART BURN
GLAUCOMA:
. PAIN
. TUNNEL VISION, HALO, GUN BARREL
. TONOMETRY
. MGT- TRABECULOPLASTY (CREATE PASSAGE OF BLOCKED FLUID)
GONORRHEA:
. BURNING ON URINATION
. ASSYMPTOMATIC ON FEMALE PT
GUILLAIN BARRE SYNDROME:
. MASK LIKE FACE
. INC CHON IN CSF
. PRIORITY- AIRWAY
HEMOPHILIA:
. HEMARTHRESIS - BLEEDING BET JOINTS
HEPATIC ENCEPHALOPATHY:
. FLAPPING TREMORS (ASTEREXIS)
. PERSONALITY CHANGES
. MGT- LACTULOSE, NEOMYCIN, DEC CHON
HERPES ZOSTER:
. PAINFUL VESICLE ALONG NERVE DISTRIBUTION
. BURNING & STABBING PAIN
HIATIAL HERNIA:
. ESRD
. UPRIGHT AFTER MEALS
HIP FRACTURE:
. RISK FOR FAT EMBOLISM
. PETECHIA OVER CHEST
HIRSCSPRUNGS DSE:
. RISK FX- MECONIUM ILEUS
HODSKINS DSE:
. PAINLESS, ENLARGED LYMPH NODES
. UNILATERAL & CERVICAL
. HODGKINS ON CHEMO- NSG DX: HIGH RISK FOR INFXN
HYATIDIFORM MOLE:
. CHORIO CARCINOMA
. DEFER PREGNANCY FOR ATLEAST ONE YR AFTER TX
HYDROCEPHALUS:
. 45 CM HEAD CIRCUMFERENCE
HYPERPARATHYROIDISM:
. RENAL STONE FORMATION
. STRAIN URINE
HYPOPARATHYROIDISM:
. TETANY
. INC CA INTAKE
HYPERTHYROIDISM:
. FINE TREMORS
. TACHYCARDIA
. PRIMARY SYMPTOM- EXOPTHALMUS
. PTU- REPORT SORE THROAT(AGRANULOCYTISIS)
. HEAT INTOLERANCE
HYPOTHYROIDISM:
. COLD INTOLERANCE
. RAPID WT GAIN
. EASY FATIGABILITY
. MED- SYNTHROID
INCREASED ICP:
. INC TEMP , INC BP
. PRESSURE OF ABOVE 150 MM/HG
. CUSHINGS TRIAD- WIDENING OF PULSE, DEC PR, DEC RR
KAPOSIS SARCOMA:
. BLUISH, PURPLE, PINKING, BRONISH DISCOLORATION
LEAD POISONING:
. PRIMARY MANIFESTATION- SEIZURE
. MORE THAN 0 MG/DL LEAD IN BLD
. MGT- IMMEDIATE HOSPITALIZATION FOR DETOX
. CALCIUM AND EDTA
LIVER CIRRHOSIS:
. ALCOHOLISM
. JAUNDICE
LIMES DSE:
. LONG TERM COMPL’N- ARTHRITIS
. DEER TICKS
. BULLS EYE RASH
MENIERES DSE:
. VERTIGO
MENIGITIS:
. PT 2 MOS BELOW- PROJECTILE VOMITTING
. ABOVE 2 MOS- NUCHAL RIGIDITY
MYSTHENIA GRAVIS:
. DIPLOPIA (PTOSIS)
. MASK LIKE FACE
. DROOPING OF EYELIDS (PTOSIS)
. DX- TENSILON TEST
. (+) MGT IF PT INC IN CHEWING
MULTIPLE SCLEROSIS:
. S/SX- DOUBLE VISION (EARLY SX), WEAKNESS IN EX, MUSCLE TREMORS
. NSG DX- INEFFECTIVE BREATHING PATTERN
. INABILITY TO DIFFERENTIATE BET HOT & COLD
. DX- MRI
MYOCARDIAL INFARCTION:
. LAB TEST- LDH
. ST SEGMENT
. BILATERAL BASILAR CRACKLES (L VENTRICULAR DYSPNEA)
. S3 GALLOP
. XYLOCAINE/LIDOCAINE
PANCREATITIS:
. AUTODIGESTION OF PANCREAS
. DIET- DEC FAT
. PERI UMBICAL PAIN
. TEST- SERUM AMYLASE (DEC SERUM LEVEL)
. DEC PRODUCTION OF INSULIN
. CHECK FOR PAIN
. MED- DEMEROL
. NSG DX- IMBALANCED NUTRITION, LESS THAN BODY REQ
PARKINSONS DSE:
. CAUSED BY DEGENERATION OF NEURONS OF THE BASAL GANGLIA
. EXPRESSIONLESS FACE (MASK LIKE)
. DROOLING
. COMMON AMONG BOXERS
. DRUG- LEVODOPA
PATENT DUCTUS ARTERIOSUS:
. (+) HEART MURMUR
. PULMONARY ARTERY IN AORTA
. MED- INDOMETHACIN
TOF (TETRALOGY OF FALLOT)
. (+) HEART MURMUR
. SQUATING- DEC CIRCULATION AND BLD VOL IN CIRCULATION
PEPTIC ULCER, DOUDENAL:
. PAINFUL
. AVOID NON-STEROID INFLAMMATORY AGENT
. RELIEVED BY EATING
PEPTIC ULCER, GASTRIC:
. LEFT SIDED PAIN
. PAIN RELIVED BY VOMITING
. BLAND DIET IS INDICATED
. SMALL FREQUENT MEALS
PHENYLKETONURIA:
. METABOLIC TEST
. GUTHRIE CAPILLARY TEST - INC CHON INTAKE 2-4 DAYS PRIOR
. LEADS TO MENTAL RETARDATION
POLYCYTHEMIA VERA:
. INC RBC LEADING TO THROMBOSIS
. INTERVENTION- PHLEBOTOMY, 500 CC OF BLOOD
PNEUMONIA:
. INC RR
. COMMON AMONG THE VERY YOUNG AND ELDERLY
POSTPARTUM HEMORRHAGE:
. RETAINED PLACENTA
. DO FUNDIC MASSAGE
PIH:
. DARKEN ROOM
. DRUG- MGSO4
. ANTIDOTE- CA GLUCONATE
PYLORIC STENOSIS:
. VISIBLE GASTRIC PERISTALTIC WAVE
. INCREASE EPI OF VOMITING
. PROJECTILE VOMITING
RENAL COLIC:
. S/SX- SEVERE FLANK PAIN NOT RELIEVED BY ANALGESICS
. STRAIN URINE
END STAGE RENAL DSE:
. CHRONIC RENAL FAILURE
. INITIAL S/SX- NAUSEA 7 VOMITING
. PRURITUS- TEPID H2O BATH
RETINAL DETACHMENT:
. VISUAL FLOATER
. VISUAL FIELD LOSS
. INTERVENTION- BEDREST
. DRUG OF CHOICE- ATROPINE SO4
RETINOBLASTOMA:
. CATS EYE REFLEX (STRABISMUS)
. REFER TO GENETICIST
REYES SYNDROME:
. AVOID ASPIRIN
RHEUMATIC HEART DSE:
. HX OF SORE THROAT
. COMPLICATION- VALVULAR HEART DSE
SALMONELLOSIS:
. HALF COOKED EGG & MEAT
SCOLIOSIS:
. UNEVEN WAISTLINE, HAIRLINE, SKIRT ETC
. NSG DX- BODY IMAGE DISTURBANCE
SIADH:
. CHECK FOR PALMAR CREASE OR SEMIAN CREASE
. CONGESTIVE HEART DSE
. SEIZURE PRECAUTION
SICKLE CELL ANEMIA:
. X LINK RECESSIVE
. 25% OF BOTH PARENT IS CARIER
. PRIMARY INTERVENTION- HYDRATION
. NSG DX- PAIN
SPINAL CORD INJURY:
. C3- C4- CHECK FOR RESPIRATORY FUNC
. PRIORITY- AIRWAY
. LOG ROLL PT WHEN MOVING
. BEST POS’N- ELEVATED, NEUTRAL HEAD ALIGNMENT, WITH NECK FLEXION ON ROTATION (DOES NOT IMPEDE OUTFLOW)
. COMPLICATION- AUTONOMIC DYSREFLEXIA
THROMBOPHLEBITIS:
. S/SX- EDEMA
. KEEP TAPE MEASURE @ BEDSIDE
ULCERATIVE COLITIS:
. L ABD’L PAIN
. FAMILIAL
. REFER TO GENETICIST
. HYPERACTIVE BOWEL SOUNDS
. S/SX- BLOODY MUCOID, DIARRHEA 15-20/DAY
THERAPEUTIC DIET
BLAND DIET:
. NO LETTUCE & SPICY FOODS
CHON RICH:
. BAKE CUSTARD
. PUMP CAKE/LECHE FLAN
HIGH NA+:
. CARROT & CELERY
LOW SODIUM:
. APPLE JUICE
LIVER CIRRHOSIS:
. LOW CHON (MEAT & POULTRY)
CYSTIC FIBROSIS:
. HIGH CALORIE, HIGH NA, HIGH CHON, LOW FAT
DUMPING SYNDROME:
. HIGH FAT, LOW CARB, DRY DIET
EDEMA:
. HIGH CHON, LOW ALBUMIN (4-6.5)
MAOI:
. FRESH VEGE AND FISH (NO PRESERVATIVES)
MANIC:
. FINGER FOODS/ MEAT SANDWICHES
ULCERATIVE COLITIS:
. NO CELERY, LETTUCE, TOMATOES
SALMONELLOSIS:
. CONTRAINDICATED- TURLTE EGGS & HALF COOKED EGG
PANCREATITIS:
. LOW FAT DIET
AGE:
. INCREASE FLUID INTAKE
GASTRIC ULCER:
. BLAND DIET
AGN:
. LOW NA, LOW CHON
NEPHROTIC SYNDROME:
. LOW NA, HIGH CHON
HYPERTHYROIDISM:
. HIGH CALORIE
ADDISONS DSE:
. HIGH NA, LOW K- VEGETABLES
CUSHINGS DSE:
. LOW NA, HIGH K- FRUITS
CHOLECYSTITIS:
. LOW FAT DIET (NO GRAVY)
CELIACS DSE:
. GLUTEN-FREE DIET
HEPARIN & COUMADIN:
. AVOID GREEN LEAFY VEGETABLES
HYPERTENSION:
. LOW NA DIET
HEPATITIS A:
. HIGH CHON, HIGH CALORIE DIET
YOGURT:
. HIGH IN CALCIUM
ACID ASH DIET:
BAKED HADDOCK
CONCEPTS ON DRUGS
ADRIAMYCIN:
. CYTOTOXIC
. INCREASE FLUID INTAKE
AMINOPHYLLINE:
. MONITOR PT FOR DYSRHYTHMIA
OXYTOXIN:
. A/R-HYPERTENSION, FLUID OVERLOAD, UTERINE TETANY
MANNITOL:
. MONITOR PT FOR
KNEE JERK REFLEX
BOWEL FUNCTION
URINE OUTPUT
HYPOTHERMIA
HYPOCALCEMIA
MAOI:
. CONTRAINDICATION
AGED CHEESE
CHEDDAR CHEESE
SWISS CHEESE
RED WINE
ANY PRESERVATIVE CONTAINING FOOD
CALCIUM GLUCONATE: (ANTIDOTE MGSO4)
. IND FOR TENTANY
VITAMIN B12:
. INC GI INTINSIC FX
FESO4:
. BEST TAKEN WITH ORANGE JUICE
. TAKEN BETWEEN MEALS
ANCEF:
. CHECK MUCOSAL EROSIONS
INDOMETHACIN:
. IND FOR PATENT DUCTUS ARTERIOSUS
SYNTHROID:
. CHECK FOR DEV OF ANGINA PECTORIS
. TACHYCARDIA
. REPORT IF ENERGY LEVEL CHANGE IND OF TOXICITY
CONGENTIN:
. ANTI-EXTRAPYRAMIDAL RXN
CEFROXITIN:
. CHECK FOR SERUM CREATININE
ISONIAZID:
. BEST TAKEN ON EMPTY STOMACH
PHENOTIAZIDE:
. IND DEMENTIA
GENTAMYCIN:
. EFFECTIVE IF URIN IS ALKALINIC
. PEAK- 30 MINS AFTER ADMIN
. TRUE PEAK- 30 MINS BE NEXT ADMIN
. S/E INCSERUM BUN & CREA LEVEL
ATROMID 500 MG:
. DI TX
RANITIDINE:
. DEC HEART BURN
LEVOTHYROXIN:
. DISCONTINUE USE 4 WKS BEFORE THYROID SCAN(I 131 UPTAKE STUDY)
b
TETANUS TOXIOD:
. BOOSTER Q 10 YRS AFTERT COMPLETE SHOT (12 YRS OLD)
ATROPINE S04:
. DECREASES SALIVATION
.BRADY CARDIA (INC HR)
CYCLOBENZAPRINE:
. MUSCLE RELAXANT (IND FOR MUSCLE & BACK PAIN)
LEVODOPA
. PARKINSON (REPORT LOSS OF APPETITE TO MD IND OF TOXICITY)
PYRAZINAMIDE:
. REPORT CHANGES IN VISION
ZIVODUVINE (AZT):
. MONITOR CBC
. C/I FLAGYL
LASIX:
. PROSTATIC HYPOTENSION
. EFFECTS ON LOOP OF HENLE
DIGOXIN:
. STRENGTHENS CARDIAC CONTRACTION
CALCIUM GLUCONATE:
. POST THYROIDECTOMY IF TETANY DEVELOPS
TAGAMET:
. TAKE ONE HR APART WITH MAALOX
COUMADIN:
. ANTI-COAGULANT
. GIVE TYLENOL NOT ASPIRIN
. MONITOR PT TIME
EPOGEN:
. INC HEMATOCRIT LEVEL
NEUPOGEN:
. INCREASE WBC COUNT
RITALIN:
. ADHD (INC ATTN SPAN)
KAVA-KAVA:
. SEDATIVE- FOR INSOMIA
ECCHINECEA:
. INC IMMUNE SYSTEM, TOPICAL, C/I FOR AIDS & TB
ST JONHS WORT:
. ANTI DEPRESSANT, C/I PREG
CORE CONCEPTS OF DRUGS
. VALIUM & AMYNOPHILLINE INCOMPATIBLE WITH OTHER DRUGS (GIVEN SEPERATELY)
. ADVERSE RXN OF MOST DRUGS INCLUDES BONE MARROW DEPRESSION
. SIDE EFFECT OF MOST DRUGS CAUSES GI DISCOMFORT
. ALWAYS NOTE DRUG THERPEUTIC LEVEL
. REMEMBER MAX DOSE AND DRUG MODIFICATION FOR ELDERLY
. NEURO & ENDOCRINE DRUGS ARE LIFETIME DRUGS
. ANTI-PSYCHOTIC DRUGS ISBEST TAKEN AFTER MEALS
<
. ANTI-ANXIETY DRUGS IS BEST TAKEN BEFORE MEALS
FUNDAMENTALS OF NURSING
NURSING PROCESS
1. Assessment
Collection & examination of data
Validation
Organization
Pattern Identification
2. Diagnosis/Problems/Needs
Analyzing data to identify
Health problems and strengths
Problem Identification (etiology)
Signs and Symptoms
3. Planning
Developing a plan of action
Implementation
Putting the plan into action
4. Evaluation
Evaluation goal achievement
Review the nursing process and update
5. Collaborative Nursing Actions
Independent nursing actions
Dependent nursing actions
NURSING PROCESS TERMINOLOGY
Data Gathering Nursing History
Intake Interview
Admission Interview
Assessment
Problem Identification Needs
Problems
Problem List
Nursing Diagnosis
Goal Setting Objectives
Short-Term Goals
Long-Term Goals
Expected Outcomes
Outcome Criteria
Criteria for Discharge
Intervention Approaches
Methods
Solutions
Nursing Orders
Plan of Action / Plan of Care
Nursing Prescriptions
MASLOW'S HIERARCHY OF HUMAN NEEDS:
Priority Ranking of Subcategories
Physiological
1. AIR: airway, breathing, gas exchange,
2. CIRCULATION: pulse, bleeding, cardiac output, tissue perfusion
3. WATER: fluid & electrolyte balance, acid-base balance
4. FOOD BALANCE: nutrition, N&V, self-care deficit: feeding
5. WASTE ELIMINATION: bowel and urinary problems, self-care deficit: toileting
6. TEMPERATURE CONTROL: skin integrity, elevated or subnormal temp, protection from infection
7. REST: sleep deprivation, disturbance of rest, need of relaxation
8. COMFORT: freedom from pain, pain avoidance
9. ACTIVITY: exercise, immobility, intolerance to activity, energy
10. CLEANLINESS: self-care deficits: grooming/hygiene
11. STIMULATION: need for sensory input, sensory overload, orientation needs, alteration in sensory perception
12. SEXUALITY: sexual dysfunction
Safety/Security Needs
1. PROTECTION FROM PHYSICAL HARM: potential for injury: falls, bruising, strange environment: (potential for
violence)
2. PROTECTION FROM PSYCHOLOGICAL THREAT: stress management, fear, spiritual well-being/comfort
3. DEPENDENCE: powerlessness, hopelessness, coping needs (individual and family), need for emotional support.
4. PREDICTABLE, ORDERLY WORLD: environmental needs
5. SECURITY: needs of self-protection through structure, law, order, and limits; example: security of a spouse or occupational position; anxiety
6. FINANCIAL SECURITY: impairment in home maintenance
7. KNOWLEDGE: need for information about disease, procedures, health maintenance for safety and security needs
Love and Belonging Needs (Social)
1. LOVE: (need for affection), alteration in parenting, ineffective individual coping, companionship needs.
2. BELONGING NEEDS: alterations in family process, ineffective family coping, aloneness, isolation, alienation
3. SOCIAL: diversional activities, socializing, privacy
Self-Esteem Needs
1. BODY IMAGE: dysfunctional grieving r/t body image changes
2. SELF-CONCEPT: high evaluation of self, sense of usefulness, sense of adequacy; diagnose and amplify
strengths
3. ESTEEM-FROM-OTHER NEEDS
4. CONTROL OVER: SELF, OTHERS, SITUATION: powerlessness
PROF ADJUSTMENT, MGT AND RESEARCH
PROF ADJUSTMENT
PROFESSIONAL- OCCUPATION BUT IT REQUIRES AN ANDVANCED SKILLS AND EXPERIENCE IN A SPECIALIZED FIELD THAT RENDERS SERVICE TO SOCIETY IN THAT SPECIAL FIELD.
CRITERIA OF A PROFESSIONAL
1. BODY OF KNOWLEDGE (EG NURSING THEORIES)
2. ONGOING RESEARCH EG NSG THEORIES
3. SPECIALIZED EDUCATION
4. SERVICE- ORIENTED (HIGHLY VALUED-ALTRUISM-SELFLESS SERVICE)
5. CODE OF ETHICS (GUIDELINE FOR MORAL CONDUCT OF NURSE)
6. AUTONOMY (INDEPENDENCE)
7. PROFESSIONAL ORGANIZATION (PNA)
RN PROFESSIONAL NURSE
A GRADUATE OF BSN
PASS THE MINIMAL REQS
PROFESSIONAL NSG- PERFORMANCE FOR A FEE
DUTIES OF A PROFESSIONAL NURSE:
PROVIDE NSG CARE USING NSG PROCESS
ESTABLISH LINKANGES W/ COMMUNITY RESOURCES AND COORDINATE WITH THE HX CARE TEAM
PROVIDE HX EDUCATION
TEACH GUIDE, SUPERVISE STAFFING AND ADMIN OF NSG SERVICE
UNDERTAKE RESEARCH + HUMAN RESOURCE DEVT
3 ARES REPRESENTED BY BON
1 CHN
2 NSG EDUC
3 NSG SERVICE
PROF EXPECTATION
1 PROPER APPEARANCE
2 AESTHETIC NEED- NEED TO BE BEAUTIFUL
3 EMPHASIS ON GOOD HEALTH
PROFESSIONAL PREP OF RN
1. BSN GRAD
2. RN
3. PHYSICALLY + MENTALLY FIT
TERMINAL COMPETENCIES
1 PROVIDE CARE USING NSG PROCESS
2 EMPLOY EFFECTIVE COMMUNICATION TECHNIGQUE
> THERA COMM
> DOCUMENTATION
3.MGT CONCEPT IN ALL LEVELS AT ANY SETTINGS
4 UNDERTAKE RESEARCH
5 RESPONSIBILITES FOR PERSONAL + PROFESSIONAL GROWTH
BEHAVIORS
1 CARING BEHAVIOR (COMPASSIONATE, COMPETENT AND COMMITED)
2 CRITICAL THINKING
3 ABILITY IN SKA
4 RESPONSIBILITY ASSUMPTION
PURPOSE OF RA 9173
- TO PROTECT THE HEALTH OF THE PUBLIC
-PREVENT PEOPLE FROM MISREPRESENTING THEMSELVES
-STATISTICS
-MOST EFFECTIVE TOOL TO CONTROL THE PROFESSION
REMOVAL OF LICENSE
SUSPENSION (TEMPORARY MAX OF 4 YRS
REVOCATION (CONFISCATE)
-- MALPRACTICE/NEGLIGENCE
--DISHONORABLE CONDUCT
--INCOMPETENT
--MISINTERPRETATION
-- 5YRS OF NON-PRACTICE
LICENSING BOARD OR BON
--1 CHAIR PERSON AND 6 MEMBERS
1 APPOINTED:1 REGULAR APPOINTMENT (TERM OF OOFICE 3 YRS)
2 AD INTERIM (SUBSTITUTE)
3 DOCTRINE OF HOLD OVER (EXTENSION OF TERM UNTIL REPLACED)
QUALIFICATIONS OF BON
1 NATURAL BORN CITIZEN
2. RN
3 MEMBER OF PNA
4. MASTERS DEGREE
FOR CHAIRPERSON
1. MAN DEGREE
MEMBERS
MSN, MAN, MPH, MA ED, ETC
>EXPERIENCE: 5-10 YRS IN THE REPUBLIC OF THE PHILIPPINES
>NOT CONVICTED OF ANY CRIME
>MUST RESIGN IN ALL NSG POSITION
>COMPENSATION- QUANTUM MERIT AS MUCH AS THEY DESERVE
REMOVAL OF A BON
1 NEGLECT OF DUTY
2 COMMISSION + TOLERANCE OF IRREGULARITIES
3 DISHONORABLE CONDUCT/ UNETHICAL
POWERS & DUTIES OF BON
1 PROMULGATE CODE OF ETHICS
2 CONDUCT LICENSURE EXAM
3 MONITOR NSG STANDARD
4 ISSUES, SUSPEND, REVOKE CERT OF REGISTRATION
5 CONDUCT HEARING AND INVESTIGATION
6 INSURE QUALITY OF NSG EDUCATION
7 SUBMIT ANNUAL REPORT TO THE PRESIDENT
8 UNDERTAKE RESEARCH AND HUMAN DEVELOPMENT
9 REPORT ANNUALLY
DUE PROCESS OF LAW
..COMPLAINANAT/PLAINTIFF
..DEFENDANT
..DISCOVERY
..TRIAL
..HEARING
..VERDICT
PRINCIPLE OF DUE PROCESS OF LAW
..PRESUMPTION OF INNOCENCE
..RIGHT TO REMAIN SILENT
..RIGHT TO A COUNSEL
..FREE ACCESS TO COURT
..AGAINST SELF INCRIMINATION
..FORCE INTIMIDATION
..INFORMED OF THE NATURE OF THE CASE
..AGAINST DOUBLE JEOPARDY
NURSE AS A WITNESS
..SUBPOENA AD TESTIFICANDUM (TESTIFY)
..SUBPOENA DUCES TECUM (DOCUMENTS)
-EXPERT WITNESS (OPINION, REFERENCER)
-WHEN TESTIFYING, A NURSE SHOULD OBTAIN AND CONSULT A LAWYER.
FIELDS OF NURSING PRACTICE
1 INSTITUTONAL /HOSPITAL NURSING
2 COMMUNITY HEALTH NURSE
3 OCCUPATIONAL HEALTH NURSE/INDUSTRIAL NURSE
4 NURSING EDUCATION
5 PRIVATE DUTYNURSE
6 CLINIC NURSE
7 SCHOOL NURSING
8 ADVANCED PRACTICE NURSING(MENTAL/PSYCHE)
9 INDEPENDENT NURSING(CRISIS MGT)
10 MILITARY NURSING
CONTRACTS
..A DOCUMENT/AGREEMENT THAT CREATES AN OBLIGATION
..MEETING OF TWO MINDS
..PERFORMANCE IN EXCHANGE FOR COMPENSATION
TYPES OF CONTRACT
. FORMAL (WRITTEN)
. INFORMAL (ORAL)
. EXPRESS- TERMS AND CONDITIONS ARE SPECIFIED
. IMPLIED (EG, EATING IN RESTO AND PAYING AFTER)
. ILLEGAL
. VIOD- INEXISTENT
REQUISITES OF CONTRACT
. TWO PARTIES
. CONSENT (MUTUAL UNSERSTANDING OF THE TERMS)
. OBJECT (SPECIFIED)
. CAUSE OF OBLIGATION MUST BE ESTABLISHED
. LEGAL CAPACITY
A. 18 YO & ABOVE
B. SOUND MIND
C. FREE FROM DURESS
D. FREE FROM INTOXICATING SUBSTANCES
E. FREE FROM DISABILITY (MENTAL RETARDATION)
ILLEGAL CONTRACTS
..MADE IN PROTECTION OF THE LAW
..OBATIN THRU FORCE OR DURESS OR UNDUE INFLUENCES
..FRAUDULENT MISINTERPRETATION
BREACH OF CONTRACT
. FAILURE OF PERFORMANCE
. FAILURE OF USE OF DUE CARE
. FAILURE OF COOPERATION
. PREVENTION OF PERFORMANCE BECAUSE OF INCONVENIENT/DIFFICULTY/SUBSTITUTION
.ABANDONMENT OF DUTY
LEGAL EXCUSES
. MISINTERPRETATION
. ILLNESS
. DEATH OF CLIENT/NURSE
. ILLEGAL PRACTICE
. INSUFFICIENT JOB DESCRIPTION
ETHICS—STUDY OF MORAL CONDUCT AND BEHAVIOR
--DISTINCTION BETWEEN RIGHT AND WRONG
CODE OF ETHICS—PROMULGATED IN 1989 BOARD RESOLUTION 1955
--BY DEAN EMIRITUS JULITA SOTEJO
FOREWORD
--HEALTH IS A FUNDAMENTAL RIGHT OF A MAN
--PRIMARY RESPONSIBILITY TO PRESERVE LIFE AT ALL COST
--PROMOTION OF HEALTH
--PREVENTION OF ILLNESS
--ALLEVIATION OF SUFFERING
--RESTORATION OF HEALTH
RESPONSIBILITIES OF A NURSE
1 NURSE TO PEOPLE
.RESPECT, VALUES, PRINCIPLE, BELIEFS
.PRIVILEGED COMMUNICATION (CONFIDENTIALITY)
2 NURSE TO PRACTICE
.MAINTAIN STANDARDS
.CLIENT ADVOCACY
3 NURSE TO COWORKER
. MAINTAIN HARMONIOUS COLLABORATIVE RELATIONSHIP
4 NURSE TO PROFESSION
. ENGAGE IN RESEARCH
. MEMBERS OF PROFESSIONAL ORGANIZATION
5 NURSE TO SOCIETY
. CONTRIBUTING MEMEBERS
PRINCIPLES OF ETHICS
DEONTOLOGY-LOGIC OF MORAL OBLIGATION: THE STUDY OF WHAT IS OBLIGATORY, PERMISSIBLE, RIGHT OR WRONG, O MORAL TERMS.
1. AUTONOMY- INDEPENDENT
-CONSENT
2. BENEFICENCE (DOING GOOD)
3. NON-MALFESCENCE (DO NO HARM)
4. JUSTICE (FAIRNESS)
5. VERACITY (TRUE FEELINGS)
6. FIDELITY (FAITHFULNESS)
7. CONFIDENTIALITY
BREACH OF CONFIDENTIALITY
A. CLIENT’S PERMISSION
B. SAFETY
C. COMMUNICABLE DISEASE
D. COMMUNICATION WITH MEMBERS OF HEALTH TEAM
MORAL RESPONSIBILITY
1. GOLDEN RULE A. CHRISTIAN-ACTIVE
B. CONFUCIANS-PASSIVE
2. TWO FOLD EFFECT (+) (-)
A. (+) WILLED
(-) MERELY ALLOWED
B. (+) MUST OUT WT THE (-)
C. ESSENTIALLY GOOD
3.EPIKA (EXCEPTION TO THE RULE)
4. ONE WHO ACTS TRU AN AGENCY IS HIMSELF RESPONSIBLE
5. PRINCIPLE OF TOTALITY (THE WHOLE IS GREATER THAN THE SUM OF ITS PART)
6. A LITTLE MORE OR LESS DOES NOT CHANGE THE SUBSTANCE OF AN ACT
7. DEFECTS OF NATURE MAYBE CORRECTED
8. PRINCIPLE OF ORIGIN AND DESTRUCTION OF LIFE (INVIOLABILITY OF LIFE)
ETHICAL ISSUES
1. AUTONOMY VS BENEFICENCE
2. CONTROVERSIAL CHOICES (ABORTION)
3. CULTURAL DIFFERENCE BET NURSE AND CLIENT
4. END OF LIFE ISSUES (DNR, ADVANCE DIRECTIVES)
5. ORGAN TRANSPLANTATION
LEGAL ASPECTS
NEGLIGENCE
A. DOING SOMETHING
B. DID NOT DO SOMETHING
TYPES OF NEGLIGENCE
1. RECKLESS IMPRUDENCE –EVIDENT-IMMEDIATE
2. EFFECTS IS DELAYED/NOT RESULT TO DAMAGE
3. SIMPLE IMPRUDENCE-DELAYED YET EVIDENT
A. MEDICATION ERRORS
B. FAILURE TO EXERT DILIGENCE
C. FAILURE TO REPORT OBSERVATION TO DOCTOR
ELEMENTS OF OF NEGLIGENCE
1. DUTY EXIST
2. BREACH OF DUTY
3. PROXIMAL USE
4. DAMAGE/INJURY
SPECIFIC ELEMENT OF NEGLIGENCE
1. FAILURE TO REPORT OBSERVATIONS TO THE DOCTOR (6 P’S)
PAIN
PALLOR
PARESTHESIA
PARALYSIS
POIKILOTHERMIA
PULSELESSNESS
2. MISTAKEN IDENTITY
3. WRONG ROUTE, DOSE, DOCUMENT, DILUTE, DRUG
4. ERRORS DUE TO FAMILY ASSISTANCE
5. FAILURE TO EXERT EFFORT THE SITUATION REQUIRES
6. FAULTY OF EQUIPMENT
LEGAL DEFENSE IN NEGLIGENCE-LEGAL DOCUMENTATION/CHART
RES IPSA LOQUITOR- THE THING SPEAKS FOR ITSELF (BURNS ETC)
FORCE MAJEURE
- NATURAL CALAMITIES
MALPRACTICE- UNSKILLFUL CARE OF THE NURSE OR STEPPING BEYOND AUTHORITY (PRESCRIBING OF MEDICATIONS)
RESPONDENT SUPERIOR- MASTER PAYS FOR THE WRONG OF SUBORDINATE.
EG DOCTOR ON MEDICATION ERROR BY NURSE
- EXPANSION OF LIABILITY
ELEMENTS
1. RELATIONSHIP BETWEEN TWO INDIVIDUALS
A. SUPERIOR
B. SUBORDINATE
2. ERROR COMMITTED BY THE SUBORDINATE
3. WORKED WAS RECEIVED FROM SUPERIOR
4. AWARENESS OR KNOWLEDGE OF THE SUPERIOR REGARDING THE SUBJECT.
INCOMPETENCE- LACK OF PHYSICAL OR MENTAL CAPACITY TO PERFORM AN ACT
LIABILITY OF NURSING AIDE
-OJT-CARE OF CHRONICALLY ILL
ROUTINE PROCEDURE (NO V/S MONITORING)
-BEDBATH
IMPROPER DELEGATION DO NOT DELEGATE
- EVALUATION
- ASSESSMENT
- TEACHING
LIABILITY OF SN
1. PREVENT ERRORS
2. PT ASSIGNED MUST BE AT THE LEVEL OF COMPETENCY
3. 1:10 STANDARD RATIO CI-STUDENT
4. FREQUENT ASSESSMENT
5. ENCOURAGE TO ASK
6. FREQUENT CONFERENCES
MEDICAL RECORDS-SCIENTIFIC + LEGAL VALUE
MEDICATIONS
-BRAND+GENRIC
NARCOTIC(YELLOW PRESCRIPTION SHEET
7 RIGHTS OF DRUGS
ALWAYS VERIFY ORDER-NEVER CARRY OUT UNDERSIGNED ORDER
TELEPHONE ORDER MUST BE RECEIVED BY RESIDENT ON DUTY
IN CASE OF EMERGENCIES MUST BE SIGNED WITHIN 24 HRS AND MUST BE WITH DATE AND NAME OF MD
INTENTIONAL TORT-HAS MOTIVE/WRONGDOING
TYPES OF TORT
1. ASSAULT
2. ILLEGAL DETENTION
3. INVASION OF PRIVACY
4. DEFAMATION OF CHARACTER/ CHARACTER ASSASSINATION
CRIME-ANY ACT IN VIOLATION OF THE LAW
ELEMENTS OF CRIME
1. CRIMINAL ACT
2. CRIMINAL INTENT
3. VOLUNTARY
CONSPIRACY-AGREEMENT BETWEEN TWO PEOPLE TO COMMIT CRIME
DEGREE OF PARTICIPATION
1. PRINCIPAL-MASTERMIND
2. ACCOMPLICE-ASSITIVE
3. ACCESSORY-HIDE THE EVIDENCE
FELONY-PUNISHABLE BY PENAL CODE
EG STEALING
TYOPES OF FELONY
1. GRAVE FELONY (AFFLICTIVE: DEATH-IMPRISONMENT 6YRS + 1 DAY)
2. LESS GRAVE (CORRECTIONAL:6YR +1 MONTH+1 DAY+P2,000-P2,000 FINE)
3. LIGHT GRAVE (ARESTO MENOR: 30 DAYS+P600)
DEGREE OF EXECUTION
1. CONSUMMATED- KILL PERSON
2. FRUSTRATED- UNFULFILLED (HARMED BUT NOT KILLED)
3. ATTEMPTED- ACTED BUT NO HARM
INCIDENTAL REPORT- AN AGENCY’S DOCUMENTATION REGARDING UNUSUAL OCCURRENCES
PRIMARY PURPOSE: RISK MANAGEMENT
GOOD SAMARITAN LAW- AN RN IS EXCUSED FROM LIABILITY IN AN EMERGENCY CASE POSTED IF THE RN COMPLIED WITH THE STANDARD OF CARE
CIRCUMSTANCES AFFECTING LIABILITY
1. JUSTIFYING-ACCORDANCE WITH THE LAW
A. SELF-DEFENSE
B. DEFENSE OF A RELATIVE
C. DEFENSE OF A STRANGER
D. LAWFUL DUTY (POLICE KILLING A KILLER)
2. EXEMPTING
A. IMBECILE, RETARDED, INSANE
B. BELOW 9 YO
C. ACCIDENT
D. FEAR
3. MITIGATING-LESSEN LIABILITY
A. BELOW 18 YO OR 70 YO ABOVE
B. PROVOCATION
C. IMMEDIATE VINDICATION (RAPE VICTIM KILLING RAPIST)
D. SURRENDERED
E. PHYSICAL DISABILITY (DEAF, DUMB, BLIND ETC)
F. PHYSICAL ILLNESS
4. AGGRAVATING- INCREASE LIABILITY
A. ABUSE OF PUBLIC OFFICE/POWER
B. INSULT OF AUTHORITY
C. PLACE OF WORSHIP
D. PRE MEDITATED (PLANNED)
E. IN CONSIDERATION OF PRIZE/REWARD
F. DISGUISE/DECEIT
G. FORCED ENTRY TO HOME (VISCONDE MASSACRE)
H. CRIME IN CALAMITIES (STEALING TO VICTIMS)
I. COMMITTING GREAT RUINS (FIRE-ARSON, TERRORISM)
5. ALTERNATIVE CIRCUMSTANCES
A. RELATION SHIP :SON KILLING FATHER-AGGRAVATING
FATHER KILLING SON-MITIGATING
B. INTOXICATION :DRUNK KILLING WITH PLAN- AGGRAVATING
DRUNK KILLING W/O PLAN- MITIGATING
C. EDUCATION (NOT EXEMPT IN RAPE, ARSON, MURDER)
INFORMED CONSENT—AUTHORIZATION
-FREE AND RATIONAL ACT
--18 YO AND ABOE
--MENTALLY ILL AND MINORS ARE NOT ALLOWED TO SIGN CONSENT
TYPE OF CONSENT
1. IMPLIED- VERBALIZATION
2. EXPRESS-CHART
WILLS- TESTEMANTARY DOCUMENTS ALLOWING CONTROL IN DISPENSING OF ASSESTS AND LIABILITIES AFTER DEATH.
TYPES
1. ORDINARY-TYPE WRITTEN WITH SIGNATURE AND NOTARIZED
2. HOLOGRAPHIC- HANDWRITTEN WITHOUT WITNESS
3. NUNCUPATIVE-ORAL AND WRITTEN
LEADERSHIP—PROCESS IF INDUCING A COOPERATIVE GROUP FOR THE PURPOSE OF A GOAL REALIZATION
QUALITIES OF A LEADER
1. AUTHORITY- A RIGHT TO EXACT AN OBLIGATION
2. GROUP ORIENTED/
TO BE CONTINUED.....
RESEARCH
MEANS:
A SYSTEMATIC (FOLLOWS A PROCESS), CRITICAL (EXCLUDE EXTRANEOUS VARIABLE) INVESTIGATION OF EMPIRICAL (“TANGIBLE-CAN BE
MEASURED AND PERCEIVED; VALUES-SPIRITUAL LIFE) DATA PERTAINING TO A PARTICULAR PHENOMENON (ANYTHING THAT CAN BE
PERCEIVED/OBSERVED + CAN BE EXPLAINED)
ETHICS ON RESEARCH
-SCIENTIFIC PURPOSE
-IMPECCABILITY (TRUTH)
-FACTUALITY
-RIGHTS OF RESEARCH OBJECTS
A. RIGHT NOT TO BE HARMED
B. RIGHT TO FULL DISCLOSURE
C. RIGHT TO SELF-DISCRIMINATION
D. RIGHT TO PRIVACY AND CONFIDENTIALITY
PURPOSE OF RESEARCH
1. DESCRIPTION
2. CORRELATIONAL
3. COMPARATIVE
4. EXPLORATORY (CAUSE)
5. EXPLANATORY (DYNAMICS OF THE CAUSE)
6. SEARCH OF A NEW KNOWLEDGE (CONCEPTUAL-PURE/BASIC)
7. SEARCH FOR NEW METHODS( APPLIED: CAN BE PRACTICAL OR PROGNOTION)
STEPS IN DOING A RESEARCH
1. DEFINITON OF THE PROBLEM
-ANYTHING THAT NEEDS A SOLUTION (INCOMPLETE INFORMATION, ABSENCE OF INFORMATION OR CONFLICTING INFO)
CRITERIA OF A RESEARCHABLE PROBLEM
a. SIGNIFICANT PROBLEM (CAN IT CONTRIBUTE)
b. FEASIBILITY ( CAN IT BE ACCOMPLISHED)
c. GENERALIZATION
d. RESEARCHABLE (EMPIRICAL; MEASURABLE)
2. DEFINE THE PURPOSE OF THE STUDY
3. REVIEW OF RELATED LITERATURE
2 TYPES OF RELATED LITERATURE
a. CONCEPTUAL (NON-RESEARCH; FROM TEXT BOOK)
b. RESEARCH LITERATURE
3 MAJOR IMPORTANCE OF RELATED LITERATURE
a. IT GIVES THE RESEARCHER’S IDEAS AND METHODS + APPROACHES FOR OWN RESEARCH
b. IT UPDATES THE RESEARCHER ON THE STATUS OF HIS STUDY
c. IT PROVIDES A BASIS FOR EVALUATING “ONE’S WORK”
4. FORMULATED HYPOTHESIS
HYPOTHESIS---IS A TENTATIVE, DECLARATIVE STATEMENT REGARDING THE CAUSE OF RELATED PHENOMENON (EDUCATED GUESS)
3 TYPES OF HYPOTHESIS
1. NON-HYPOTHESIS- (X RELATIONSHIP
2. ALTERNATIVE-(HAS RELATIONSHIP
3. DIRECTIONAL-(HAS RELATIONSHIP AND DIRECTION)
VARIABLES
CAUSE
INDEPENDENT
DEPENDENT
EFFECT
E.G.-"THE EFFECTS OF MUSIC TO CLIENTS WITH POSTPARTUM BLUES”
5. SELECT RESEARCH METHODOLOGY
RESEARCH DESIGN:
a. EXPERIMENTAL
-MANIPULATION
-CONTROL
-RANDOMINAZATION
-MEASUREMENTS OF EFFECT
• QUASI-EXPERIMENTAL- DIDN’T PERFORM THE 4 FUNCTION
b. NON-EXPERIMENTAL
a. HISTORICAL- GATHERING EVIDENCES FROM THE PAST; FROM OLD BOOKS, NEWSPAPER, JOURNALS AND ARTICLE.
b. CASE STUDY-IN DEPTH ANALYSIS OF SINGLE CASE
c. SURVEY:
SUBJECTS: MASS
GROUP
METHOD: MAILED
FACE TO FACE INTERVIEW
TELEPHONE
TIME ORIENTATION: *CROSS SECTIONAL
( ONE MOMENT OF TIME)
*LONGITUDINAL
(“THROUGH THE YEARS” )
6. SELECT POPULATION AND SAMPLE
• POPULATION-- GROUP TO BE STUDIED
• SAMPLE--SCIENTIFIC GROUP WHICH DATA WILL BE COLLECTED
2 TYPES OF SAMPLING
1. RANDOM / PROBABILITY
A. SIMPLE RANDOM (EQUAL CHANCE)
B. SYSTEMATIC (EQUAL DISTANCE BETWEEN SAMPLE)
C. STRATIFIED(HOMOGENOUS SAMPLE BY GROUPS)--DIVIDED
D. CLUSTER(HETEROGENEOUS SAMPLE BY GROUP)-E.G.BARANGAY
2. NON-RANDOM / NON PROBABILITY
a. ACCIDENTAL / INCIDENTAL OCCURRENCE
b. PURPOSAL (CRITERION)
c. SNOWBALL (NETWORKING—PAY IT FORWARD)
d. QUOTA (SET LIMIT)
E.G. “ 7 OUT OF 10 MOTHER ARE BREASTFEEDING THEIR BABIES”
• SAMPLE FRAME- COMPLETE LIST OF SAMPLE
7. CONDUCT PLOT STUDIES
8. COLLECT DATA
a. INTERVIEW
2 TYPES OF INTERVIEW
1. STRUCTURE
2. UNSTRUCTURE
b. RECORDS
c. OBSERVATION
4 TYPES OF OBSERVATION
1. STRUCTURED
2. UNSTRUCTURED
3. PARTICIPANTS
4. NON-PARTICIPANTS
9. ANALYSIS AND INTERPRET DATA
MEASUREMENT OF EFFECT
a. VALIDITY
b. RELIABILITY( CONSISTENCY OF RESULT)
2 TYPES OF ANALYSIS
1. QUALITATIVE
2. QUANTITATIVE
10. COMMUNICATE RESULT
VARIABLE( PUBLISHED)
-NARRATIVE
-GRAPH
-CHARTS
-DIAGNOSIS
LEGAL ASPECT OF NURSING
ANSWER
(LEGAL) A WRITTEN RESPONSE MADE BY THE DEFENDANT
ASSAULT
AN ATTEMPT OR THREAT TO TOUCH ANOTHER PERSON UNJUSTIFIABLY
BATTERY
THE WILLFUL OR NEGLIGENT TOUCHING OF A PERSON (OR THE PERSON'S CLOTHES OR EVEN SOMETHING THE PERSON IS CARRYING), WHICH MAY OR MAY NOT CAUSE HARM
BREACH OF DUTY
A STANDARD OF CARE THAT IS EXPECTED IN THE SPECIFIC SITUATION BUT THAT THE NURSE DID NOT OBSERVE; THIS IS THE FAILURE TO ACT AS A REASONABLE, PRUDENT NURSE UNDER THE CIRCUMSTANCES
BURDEN OF PROOF
THE DUTY OF PROVING AN ASSERTION
CAUSATION
A FACT THAT MUST BE PROVEN THAT THE HARM OCCURRED AS A DIRECT RESULT OF THE NURSE’S FAILURE TO FOLLOW THE STANDARD OF CARE AND THE NURSE COULD HAVE (OR SHOULD HAVE) KNOWN THAT FAILURE TO FOLLOW THE STANDARD OF CARE COULD RESULT IN SUCH HARM
CIVIL ACTION
DEALS WITH THE RELATIONSHIP BETWEEN INDIVIDUALS IN SOCIETY
CIVIL LAW
THE BODY OF LAW THAT DEALS WITH RELATIONSHIPS AMONG PRIVATE INDIVIDUALS; ALSO KNOWN AS PRIVATE LAW
COMMON LAW
THE BODY OF PRINCIPLES THAT EVOLVES FROM COURT DECISIONS
COMPLAINT
(LEGAL) A DOCUMENT FILED BY THE PLAINTIFF
CONTRACT
A WRITTEN OR VERBAL AGREEMENT BETWEEN TWO OR MORE PEOPLE TO DO OR NOT DO SOME LAWFUL ACT
CONTRACT LAW
THE ENFORCEMENT OF AGREEMENTS AMONG PRIVATE INDIVIDUALS OR THE PAYMENT OF COMPENSATION FOR FAILURE TO FULFILL THE AGREEMENT
CONTRACTUAL OBLIGATIONS
DUTY OF CARE ESTABLISHED BY THE PRESENCE OF AN EXPRESSED OR IMPLIED CONTRACT
CONTRACTUAL RELATIONSHIPS
VARY AMONG PRACTICE SETTINGS; MAY BE AS AN INDEPENDENT OR EMPLOYER-EMPLOYEE RELATIONSHIP
CREDENTIALING
THE PROCESS OF DETERMINING AND MAINTAINING COMPETENCE IN PRACTICE; INCLUDES LICENSURE, REGISTRATION, CERTIFICATION, AND ACCREDITATION
CRIME
AN ACT COMMITTED IN VIOLATION OF PUBLIC (CRIMINAL) LAW AND PUNISHABLE BY A FINE AND/OR IMPRISONMENT
CRIMINAL ACTION
DEALS WITH DISPUTES BETWEEN AN INDIVIDUAL AND THE SOCIETY AS A WHOLE
CRIMINAL LAW
DEALS WITH ACTIONS AGAINST THE SAFETY AND WELFARE OF THE PUBLIC
DAMAGES
IF MALPRACTICE CAUSED THE INJURY, THE NURSE IS HELD LIABLE FOR DAMAGES THAT MAY BE COMPENSATED
DECISION
(LEGAL) OUTCOME MADE BY A JUDGE
DEFAMATION
(LEGAL) A COMMUNICATION THAT IS FALSE, OR MADE WITH CARELESS
DISREGARD FOR THE TRUTH, AND RESULTS IN INJURY TO THE REPUTATION OF ANOTHER
DEFENDANT
(LEGAL) PERSON AGAINST WHOM THE PLAINTIFF FILES A COMPLAINT AGAINST
DELEGATION
TRANSFERRING TO A COMPETENT INDIVIDUAL THE AUTHORITY TO PERFORM A SELECTED NURSING TASK IN A SELECTED SITUATION
DISCOVERY
(LEGAL) PRETRIAL ACTIVITIES TO GAIN ALL THE FACTS OF THE SITUATION
DUTY
THE NURSE MUST HAVE (OR SHOULD HAVE HAD) A RELATIONSHIP WITH THE CLIENT THAT INVOLVES PROVIDING CARE AND FOLLOWING AN ACCEPTABLE STANDARD OF CARE
EXPERT WITNESS
ONE WHO HAS SPECIAL TRAINING, EXPERIENCE, OR SKILL IN A RELEVANT AREA AND IS ALLOWED BY THE COURT TO OFFER AN OPINION ON SOME ISSUE WITHIN THAT AREA OF EXPERTISE
EXPRESS CONSENT
AN ORAL OR WRITTEN AGREEMENT
FALSE IMPRISONMENT
THE UNLAWFUL RESTRAINT OR DETENTION OF ANOTHER PERSON AGAINST HIS OR HER WISHES
FELONY
A CRIME OF A SERIOUS NATURE, SUCH AS MURDER, PUNISHABLE BY A TERM IN PRISON
FORESEEABILITY
A LINK THAT MUST EXIST BETWEEN THE NURSE’S ACT AND THE INJURY SUFFERED
GROSS NEGLIGENCE
INVOLVES EXTREME LACK OF KNOWLEDGE, SKILL, OR DECISION MAKING THAT THE PERSON CLEARLY SHOULD HAVE KNOWN WOULD PUT OTHERS AT RISK FOR HARM
HARM
THE CLIENT OR PLAINTIFF MUST DEMONSTRATE SOME TYPE OF HARM OR INJURY (PHYSICAL, FINANCIAL OR EMOTIONAL) AS A RESULT OF THE BREACH OF DUTY OWED THE CLIENT. THE PLAINTIFF WILL BE ASKED TO DOCUMENT PHYSICAL INJURY, MEDICAL COSTS, LOSS OF WAGES, "PAIN AND SUFFERING," AND ANY OTHER DAMAGES
IMPAIRED NURSE
A NURSE WHOSE PRACTICE HAS DETERIORATED BECAUSE OF CHEMICAL ABUSE
IMPLIED CONSENT
CONSENT THAT IS ASSUMED IN AN EMERGENCY WHEN CONSENT CANNOT BE OBTAINED FROM THE CLIENT OR A RELATIVE
IMPLIED CONTRACT
A CONTRACT THAT HAS NOT BEEN EXPLICITLY AGREED TO BY THE PARTIES BUT THAT THE LAW NEVERTHELESS CONSIDERS TO EXIST
INFORMED CONSENT
A CLIENT'S AGREEMENT TO ACCEPT A COURSE OF TREATMENT OR A PROCEDURE AFTER RECEIVING COMPLETE INFORMATION, INCLUDING THE RISKS OF TREATMENT AND FACTS RELATING TO IT, FROM THE PHYSICIAN
INJURY
SEE HARM
INTERSTATE COMPACT
INVASION OF PRIVACY
A DIRECT WRONG OF A PERSONAL NATURE, IT INJURES THE FEELINGS OF THE PERSON AND DOES NOT TAKE INTO ACCOUNT THE EFFECT OF REVELED INFORMATION ON THE STANDING OF THE PERSON IN THE COMMUNITY
LAW
A RULE MADE BY HUMANS THAT REGULATE SOCIAL CONDUCT IN A FORMALLY PRESCRIBED AND BINDING MANNER
LIABILITY
THE QUALITY OR STATE OF BEING LEGALLY RESPONSIBLE FOR ONE’S OBLIGATIONS AND ACTION AND TO MAKE FINANCIAL RESTITUTION FOR WRONGFUL ACTS
LIBEL
DEFAMATION BY MEANS OF PRINT, WRITING, OR PICTURES
LICENSE
A LEGAL PERMITS GRANTED TO INDIVIDUALS TO ENGAGE IN THE PRACTICE OF A PROFESSION AND TO USE A PARTICULAR TITLE
LITIGATION
THE ACTION OF A LAWSUIT
MALPRACTICE
THE NEGLIGENT ACTS OF PERSONS ENGAGED IN PROFESSIONS OR OCCUPATIONS IN WHICH HIGHLY TECHNICAL OR PROFESSIONAL SKILLS ARE EMPLOYED
MANDATED REPORTERS
A ROLE OF THE NURSE IN WHICH HE OR SHE IDENTIFIES AND ASSESSES CASES OF VIOLENCE AGAINST OTHERS, AND IN EVERY CASE THE SITUATION MUST BE REPORTED TO THE PROPER AUTHORITIES
MANSLAUGHTER
SECOND DEGREE MURDER
MISDEMEANOR
A LEGAL OFFENSE USUALLY PUNISHABLE BY A FINE OR A SHORT-TERM JAIL SENTENCE, OR BOTH
MUTUAL RECOGNITION MODEL
A NEW REGULATORY MODEL DEVELOPED BY THE NATIONAL COUNCIL OF STATE BOARDS OF NURSING (NCSBN), WHICH ALLOWS FOR MULTISTATE LICENSURE
NEGLIGENCE
FAILURE TO BEHAVE IN A REASONABLE AND PRUDENT MANNER; AN UNINTENTIONAL TORT
PLAINTIFF
A PERSON CLAIMING INFRINGEMENT OF LEGAL RIGHTS BY ONE OR MORE PERSONS
PRIVATE LAW
(CIVIL LAW) THE BODY OF LAW THAT DEALS WITH RELATIONSHIPS BETWEEN PRIVATE INDIVIDUALS
PUBLIC LAW
REFERS TO THE BODY OF LAW THAT DEALS WITH RELATIONSHIPS BETWEEN INDIVIDUALS AND THE GOVERNMENT AND GOVERNMENTAL AGENCIES
RES IPSA LOQUITUR
"THE THING THAT SPEAKS FOR ITSELF"; A LEGAL DOCTRINE THAT RELATES TO NEGLIGENCE IN WHICH THE HARM CANNOT BE TRACED TO A SPECIFIC HEALTH CARE PROVIDER OR STANDARD BUT DOES NOT NORMALLY OCCUR UNLESS THERE HAS BEEN A NEGLIGENT ACT
RESPONDEAT SUPERIOR
A LEGAL TERM MEANING "LET THE MASTER ANSWER"; THE EMPLOYER ASSUMES RESPONSIBILITY FOR THE CONDUCT OF THE EMPLOYEE AND CAN ALSO BE HELD RESPONSIBLE FOR MALPRACTICE BY THE EMPLOYEE
RIGHT
A PRIVILEGE OR FUNDAMENTAL POWER TO WHICH AN INDIVIDUAL IS ENTITLED UNLESS IT IS REVOKED BY LAW OR GIVEN UP VOLUNTARILY
RESPONSIBILITY
THE OBLIGATION ASSOCIATED WITH A RIGHT
SLANDER
DEFAMATION BY THE SPOKEN WORD, STATING UNPRIVILEGED (NOT LEGALLY PROTECTED) OR FALSE WORDS BY WHICH A REPUTATION IS DAMAGED
STANDARDS OF CARE
DETAILED GUIDELINES DESCRIBING THE MINIMAL NURSING CARE THAT CAN REASONABLY BE EXPECTED TO ENSURE HIGH QUALITY CARE IN A DEFINED SITUATION (EG, A MEDICAL DIAGNOSIS OR A DIAGNOSTIC TEST)
STATUTORY LAW
A LAW ENACTED BY ANY LEGISLATIVE BODY
STRIKE
AN ORGANIZED WORK STOPPAGE BY A GROUP OF EMPLOYEES TO EXPRESS A GRIEVANCE, ENFORCE A DEMAND FOR CHANGES IN CONDITION OF EMPLOYMENT, OR SOLVE A DISPUTE WITH MANAGEMENT
TORT
A CIVIL WRONG COMMITTED AGAINST A PERSON OR A PERSON'S PROPERTY
TORT LAW
LAW THAT DEFINES AND ENFORCES DUTIES AND RIGHTS AMONG PRIVATE INDIVIDUALS THAT ARE NOT BASED ON CONTRACTUAL AGREEMENTS
TRIAL
THE PERIOD DURING WHICH ALL THE RELEVANT FACTS ARE PRESENTED TO A JURY OR JUDGE
UNPROFESSIONAL CONDUCT
ONE OF THE GROUNDS FOR ACTION AGAINST THE NURSE'S LICENSE; INCLUDES INCOMPETENCE OR GROSS NEGLIGENCE, CONVICTION OF PRACTICING WITHOUT A LICENSE, FALSIFICATION OF CLIENT RECORDS, AND ILLEGALLY OBTAINING, USING OR POSSESSING CONTROLLED SUBSTANCES
VERDICT
THE OUTCOME MADE BY A JURY
